Co-Editors: Lisa Sokoloff, LCSW
William Goldberg, LCSW
|
|
Let’s Look at Culture
Lorna Goldberg, L.C.S.W., Psy.A.
Director, Institute for Psychoanalytic Studies
|
I am an older female Jewish clinical social worker/psychoanalyst from New Jersey. I suspect that those who don’t know me will form an instant snapshot of who I am based upon reading this. We tend to have impressions of each other according to affiliations that are seen through our own cultural filters. In
Group Psychology and the Analysis of the Ego, Freud theorized that, in groups, we develop an ego ideal and this contributes to our sense of belonging and our group identity (Freud, 1921).
However, as Freud also indicated, narcissism of minor differences reinforces both our group identity and our need for an outsider in an attempt to keep aggressive feelings outside our group (Freud, 1929-1930).
At the same time, our own unique experiences (and the meaning that we’ve given to those experiences) shape our cultural biases. We need to consider that outward images of others also involve a refinding of images that are found within (Freud, 1905). While this is a time in this country and in the world when ethnocentrism is heightened, therapists might consider that, instead seeing cultural differences simply as a tool to claim superiority over others, exploration of cultural differences can be the starting point for gaining insight into our own and our patients’ biases and inner beliefs.
At the Institute for Psychoanalytic Studies, our students and faculty come from Central and South America, Asia, and Europe as well as from Canada and the United States. We are different religions and races. In our courses, our cultural differences expand the learning process for all of us. As we study together in our courses, students and faculty have the opportunity to bring their unique perspectives of their experiences in the wider world to the intrapsychic material at hand.
When teaching about different developmental theories, it’s also helpful to learn about the theorists themselves and, particularly, understand the culture in which they lived to gain insight into how this might have impacted their theoretical perspective. For example, how did the Victorian model of acceptable feminine behavior (which restricted the feminine role outside the home for many and emphasized female chastity) influence Freud’s patients’ symptomatology and, subsequently, influence Freud’s theory of sexual differences? Although Freud’s views of biological gender and sexual considerations continue to be valid for some girls today, how do newer theories modify Freud’s thinking, providing us with additional ways of looking at female development? For example, in 1997, Galenson and Roiphe modified Freud’s theory to include a continuum of female reactions to sexual differences; and, in 2000, Holzman and Kulish expanded the notion of Oedipal reactions for girls by writing,
We have found that issues of mother-daughter separation are a fundamental part of the female oedipal
paradigm. For that reason, we feel that the triangular phase for girls is not well characterized by the
Oedipus myth, and propose renaming it the ‘Persephone complex.’ Persephone's compromise between
innocence and sexuality, her conflicting loyalties to her mother and her father, and her means of traversing
the boundary between childhood and adulthood typify for us central aspects of female development
(p. 1434).
I wonder about the way in which cultural experiences and attitudes enter into the transference and countertransference dynamics of therapy. With differing cultures, there is the potential for certain transference expectations that might not be true, such as assumptions about the therapist’s attitude towards childrearing or proper behavior with family members. There also is the expectation of shared definitions of words used in our sessions together. For example, a religious woman contacted me for therapy and asked whether or not I was “spiritual.” Over the phone, I needed to explore what she meant by this term.
How do cultural differences affect our actions, fantasies, and defenses? Many years ago, I worked with a depressed woman who set a fire in her washing machine, which resulted in the destruction of her suburban home. This initially might have appeared as the act of a psychotic woman, and I initially felt apprehensive about working with this patient based upon my expectations about who she would be. However, in therapy, I learned that this intelligent and eloquent woman had panicked, never expecting her small fire to become so large and destructive. I also learned that she had come to New Jersey from India to marry a virtual stranger and she was incredibly lonely and depressed living in her new home, far away from her family. It also was important for me to learn that, for my patient, the act of fire setting in India as a result of depression was not seen as pathological as it was seen in the United States. For example, in India, at times, fire setting has been seen as a form of protest; and, also, for many years, there was the practice of Sati, in which a widow falls on her husband’s funeral pyre. My point is that, just as we need to allow for many theoretical possibilities when we listen to our patients, we need to allow for the influence cross-cultural differences and biases in relation to normal and abnormal behavior. When we attempt to understand how culture influences our patients, we amplify a feeling of shared understanding and, at times, we diminish feelings of shame. Experiencing my attempt to understand my patient in our therapy sessions contrasted with her experiences with police and others after this incident occurred. We can see character as circular with our inner life affecting our worldviews and outer life experiences affecting inner life fantasies and conflicts.
Psychoanalysis has helped me understand that things aren’t necessarily as we perceive them to be. In order not to be locked into one belief system, analysis provides each of us with a method for self-reflection. It allows us to gain a deeper understanding of ourselves and to discover our own biases and to better understand the potential biases of others.
Joel Bernstein, our founder, described the importance of exploring our patient’s character traits, picked up through our induced countertransference feelings, within the treatment process. When we do so, we discover how our patients’ inborn temperaments can interact with their fantasy life to shape memories of the past. This exploration, beginning in the therapy room with our induced reactions to our patients, leads us to the possibility of differing theories that help us better understand what we are seeing, hearing, and feeling. Therefore, for all of us, childhood is a time in which character is shaped from the meaning we make of our early experiences, influenced by cultural differences as well as by constitutional factors and developmental stages.
References
Freud, S. (1955).
Group psychology and the analysis of the ego. In J. Strachey (Ed. and trans.),
The standard edition of the compete psychological works of Sigmund Freud, 18 (pp. 65-143). London, England: Hogarth Press. (Original work published 1921).
Freud, S. (1955).
Civilization and its discontents. In J. Strachey (Ed. and trans.)
The standard edition of the complete psychological works of Sigmund Freud, 21 (59-145). London, England: Hogarth Press. (Original work published in 1929-1930).
Freud, S. (1955).
Three essays on sexuality. In J. Strachey (Ed. and trans.)
The standard edition of the complete psychological works of Sigmund Freud, 7 (125-244). London, England: Hogarth Press. (Original work published in 1905).
Galenson, E. and Roiphe, H. (1976). Some Suggested Revisions
Concerning Early Female Development.
Journal of the American Psychoanalytic Association, 24(S): 29-57.
Holtzman, D. & Kulish, N. (2000). The feminization of the female oedipal complex: Part I. A reconsideration of the significance of separation issues.
Journal of the American Psychoanalytic Association. 48:1413-1437.
|
|
Faculty Member Joyce Grossbard Travels to Japan to Treat Trauma Victims
|
|
Joyce with Japanese survivors
|
On March 11, 2011, the most powerful earthquake ever recorded in Japan struck off Japan’s northeastern shore, generating enormous tsunami waves that spread across miles of shoreline. Damage to the reactors at a Nuclear Power Plant then caused a third disaster, contaminating a wide area that still forces nearly 100,000 residents to live as evacuees.
It happened seven years ago--20,000 lives were lost, 2,500 are still missing and over 100,000 children were orphaned. These numbers do not reflect the aftermath of the disaster in which many people took their own lives which continues to today. As time has passed, the mental health crisis has deepened as people become hopeless and severely depressed, drink, gamble, abuse their children, and live alone waiting to die.
Joyce Grossbard, IPS faculty member, went to Japan in 2013 as part of an outreach program through the Englewood Rotary Club to help address the mental health crisis that developed as a result of these traumatic events. Part of the challenge, she noted, is that the Japanese culture doesn’t encourage talking about feelings and there are very few mental health resources available in the country.
Joyce used her extensive background and training in child psychotherapy help the children heal from this devastating experience. In addition to teaching breathing techniques that calm the nervous system, Joyce developed a Memory Box Project for the children in temporary housing who had lost everything. The Memory Box, she explains, “gave them one small place of their own to preserve their good memories and to help these traumatized children in healing from the chaos that surrounded them. We wanted to connect them to the outside world that cares about them.”
|
|
A Memory Box with beach stones collected by children in the United States on which were written “hope, memory and friendship.” The inscriptions were rendered in both English and Japanese.
|
|
The children each received a special pen that writes on wood to personalize their boxes. They are all wearing their “power bracelets” that Joyce designed and had made before the trip. This was to bind them together with all of us so that even after we were gone we would all be connected to each other.
|
|
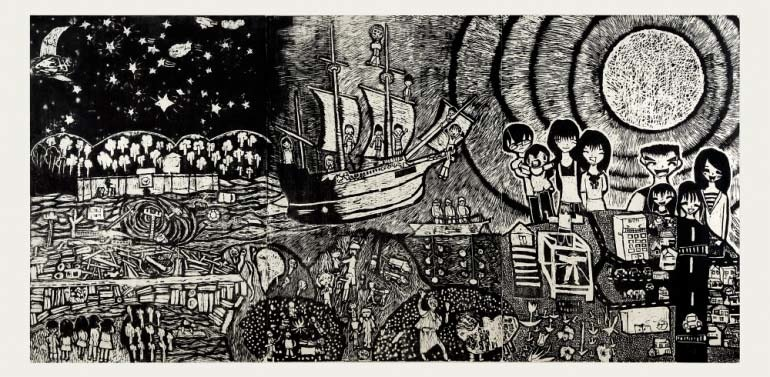
“The Ship of Hope” created by fifth-grade students in Japan who were affected by the earthquake. They watched from high on a hillside as their homes, their school and their dreams were smashed and swallowed up by the sea.
|
While in Japan, Joyce heard about the story of an elementary school teacher who developed a program called ‘Reconstructive Education’ using art as a medium for therapeutic repair.
In this program, the class carved a six-foot long woodblock depicting “The Ship of Hope,” a project that was completed after 18-months of work. The woodblock has “become a symbol of the resilience and hope for the children of Japan,” Joyce explained, and illustrates the tremendous healing potential of art and creativity to help trauma survivors process their feelings and move forward in their lives. This is the only copy of the children’s artwork and it was entrusted to Joyce. It will be displayed at the 3/11 Memorial in New York City until 2021 .
Joyce reported that the main fear of survivors is that they will be forgotten. Here’s a poem by a young girl who survived the tsunami.
I Won’t Forget
I won’t forget
that I squatted down and shook
because of the sound of the earthquake
I won’t forget the old man at the gas station
who ran to save me
I won’t forget the houses that were completely destroyed and washed away
I won’t forget the precious necklace my mother gave me
and that all of our family photos were swallowed up.
I wont forget the goodness of people and the gratitude that I feel that I was saved.
To maintain the connection and fulfill her promise that they will not be forgotten, Joyce has visited Japan every summer since 2013 to meet with the same group of survivors.
|
|
Conversation
:
Manifestations of Magical Thinking in Therapy
Presenter: William Goldberg, LCSW, PsyA
Magical thinking is the belief that our private thoughts, desires or ideas can influence the external world. For some people, magical thinking is a concomitant of pathology such as psychosis or an obsessive/compulsive disorder. However, it is normal for children to employ magical thinking when they wish upon a star or when they believe that unfortunate events are the result of their secret thoughts. Although, as they mature, most healthy individuals consciously replace their magical thinking with concepts of logic and cause and effect, vestiges of this unconscious pattern may still be manifested as a reaction to stress. In this conversation, participants will discuss ways that our clients may display magical thinking and how we can help them to recognize this phenomenon.
Sunday, June 3, 2018
Five Star Premier Residence
655 Pomander Walk
Teaneck, NJ 07666
11:00 am to 1:00 pm
Conversation
:
Negotiating and Understanding the Rise of Technology in Therapy
Presenter: Zachary Schwartz, LCSW, PsyA
When Freud originally paved the way for modern day psychotherapy, he never had to contend with the internet, cell phones, email and texting. In our current clinical landscape, the world of technology has created unexpected new challenges that need to be negotiated when conducting therapy with our clients. In addition to expectations that therapists become familiar with technology, we also have to make thoughtful determinations about how and when to intervene in this new environment. As we become comfortable in navigating these situations through our clinical application and processing of technology in treatment, this process can also be instructive and allow greater understanding of our clients’ character traits. This Conversation is designed to explore how therapists deal with various aspects of the use of technology in clinical practice with our clients.
Sunday, September 16, 2018
Five Star Premier Residence
655 Pomander Walk
Teaneck, NJ 07666
11:00 am to 1:00 pm
|
|
Cultural Corner
Between Us: A Psychotherapy Podcast
Psychotherapists John Totten and Mason Neely created a psychotherapy podcast that explores what is happening between therapists and patients, from both sides of the relationship.
Here is a link to an interview with Galit Atlas, psychoanalyst and author of “The Enigma of Desire: Sex, Longing and Belonging in Psychoanalysis.”
Podcast on Science of Mindfulness
Here is a link to her interview on the subject:
“Your task is not to seek for love, but merely seek and find all the barriers within yourself that you have built against it.”
—Rumi
The Silence: The Legacy of Childhood Trauma
by Junot Diaz
Junot Diaz, a Pulitzer prize-winning author, wrote a moving personal essay in the New Yorker about his childhood sexual abuse. He recounts how this trauma affected all aspects of his life and illustrates how shame and secrets can do serious damage to the development of a self. Diaz relates that, after trying to commit suicide, he finally sought therapy, an ongoing process which helped him begin to put his demons to rest.
Here is the link:
|
|
Conversation: #METOO
Lisa Sokoloff, LCSW, PsyA
On Sunday, January 29, 2018, IPS hosted a packed room full of clinicians who wanted
to discuss the #MeToo movement and how it affects our work with patients. The Conversation was led by Lisa Sokoloff. The group discussed our
ability to “not know” as well as how dissociation can be used to wipe away a memory too painful to absorb as a way of protecting the self from being overwhelmed. The conversation covered a lot of ground - men feeling guilty about their fears of what they may have done, fantasies that can be confused with reality, how the climate of women speaking out made it possible for clients to open up and even allow themselves to remember past abuse, and how expectations for women’s sexuality were different in the past. There was a lively discussion about how the culture seems to be changing and many points
of view were expressed, including the following: Do some women want to be seen as victims? Do others who were abused want to deny their experiences?
What about women predators and males who are victims?
There wasn’t enough time to address
all the aspects of this timely discussion and we agreed that
the conversation
should continue.
Movie Night: Lion
Margaret Debrot, LCSW, PsyA
On Sunday, February 11, 2018, the Institute sponsored the first of our Movie Nights, as members of our Institute and other mental health professionals viewed and discussed the 2016 film,
Lion. The discussion was led by Cathy Lawrence and myself.
Lion is based on the true story of a five year old Indian boy named Saroo, who is lost and separated from his family in India. He is eventually adopted by an upper middle class Australian couple. Twenty-five years later, after he spends four years searching for his birth-mother on Google Earth, Saroo is re-united with his birth-mother and biological sister.
After watching the film, participants discussed the psychological dynamics of Saroo and his search for his biological family. Among the topics touched upon were the following: Freud’s theories of repression and the return of the repressed; the inborn temperament of infants; the character of the Saroo and how that character helped him to survive; trauma as it related to individuals who grew up in Uganda; ambivalent feelings expressed by Saroo in his relationships, which may have been a projection of inner conflicts and pain; resilience in people.
According to the feedback forms, the participants found the discussion to be informative and helpful. We plan to have more Movie Nights and Discussions in the future.
Conversation: Self Disclosure in Therapy
Thomas Grace, PsyD, PsyA
On March 18, 2018, The Institute for Psychoanalytic Studies was host for a lively and thought-provoking conversation about aspects of self-disclosure of countertransference reactions and personal information by the analyst. Through the recollection of personal experiences, we explored how sharing our personal experiences might enhance and impede the therapeutic process.
We began the discussion by identifying two aspects of “deliberate” self-disclosure; the analyst expressing induced reactions to a patient, and the analyst sharing personal details. Participants went on to clarify that the therapeutic value, efficacy, and safety of an analyst’s self-disclosure is simultaneously dependent on the clinical needs and wellbeing of patients, as well as the impulses and intentions driving analysts to disclose. The processes of character analysis might be further enhanced, and ruptures healed by follow up exploration of patients’ reactions and fantasies to analysts’ disclosures. The safety of a healthy therapeutic relationship, not a formula, affords rich opportunities to identify the energy and pervasiveness of needs, frustrations, and character traits.
As for “unintended” disclosure of personal information, it might not be possible to completely avoid self-disclosure as we leave traces of ourselves in choices we make, how we present ourselves, and the therapeutic environments we create. Nevertheless, there can be boundary-crossing and vulnerability-inducing risks that occur when patients dig through the online activities of an analyst to actively discover personal details without the analyst’s intention or consent for the patient to know.
If a goal of analytic treatment is to help patients to identify and disclose previously unknown and vulnerable aspects of themselves (e.g., aggressive and sexual fantasies and impulses) and then more freely choose how or if to use what they learn, then might it be possible that we as analysts can provide an important frame of reference and practice ground for our patients when we afford ourselves the possibility of using self-disclosure as clinically indicated. If we as analysts happen to benefit from that process, maybe that’s a good thing too. Thank you to all participants for your contributions. I believe we all benefitted from each other.
|
|
PSYCHOANALYSIS AND YOU: Some Questions
|
This is a new feature of the newsletter that asks candidates and members to answer a few questions about their experiences practicing psychoanalysis. Since the IPS community is notable for its diversity of candidates and members with wide-ranging backgrounds, it's interesting to hear from therapists about their different perspectives and routes to becoming psychoanalysts. Below are answers to these questions by a candidate and faculty member.
What sparked your interest in psychoanalysis?
I have always had an innate interest in getting to know people and the underlying factors/experiences that attribute to cognitions and behaviors.
What's been most challenging in learning how to become an analyst?
One of the most challenging aspects of becoming an analyst for me is the internal process of “feeling versus thinking” when sitting with the patient.
How has it changed your work (and yourself)?
Oh wow, it has lessened tremendously the expectation of myself as a therapist to produce immediate change in the patient’s cognitions as well as normalize the awareness for the therapeutic relationship that “real change(s)” takes time.
Would you recommend institute training and why?
Yes, I most definitely would for therapists who are willing to be open-minded and “unlearn” much of what they are used to when working with patients.
Do you have a specialty or preferred population and why?
I like working with older teenagers and adults who are interested in obtaining a deeper understanding of themselves over time.
How do you spend your leisure time when not in the consulting room?
My time outside the office is spent fulfilling the requirements of the Institute (i.e. attending supervision, analysis, and class), with my family (husband and 2 adult daughters), in prayer with God, watching K-dramas and Grey’s Anatomy and “cautiously” keeping up with the news:).
Rosenna Pemberton
4
th
year candidate
----------------------------------------------------------------------------------------------------------------------------
What sparked your interest in psychoanalysis?
I owe that development to my wife and the amazing community of people at IPS. Honestly, my interest and appreciation for psychoanalysis didn’t begin until well after I began studying at IPS. For some time, I had no clear theoretical orientation. I couldn’t even proclaim that I was eclectic. I knew I was not interested in nor did I have the capacity to remember any of the strategies and rules of CBT. I knew I wanted to help people, but even after earning my degree I had no substantive ideas how that was going to happen. Then, at a time that I needed a supervisor for licensure, Nicole introduced me to Joel and Lorna and just kept taking incremental steps. Even though I didn’t begin with a burning desire to become a psychoanalyst, the classes, collegial conversations, and my own work loosened resistances, and something clicked into place for me. I discovered so many remarkable and elegant truths about character, pathology, and how the honesty, compassion, and artfulness of character/psychoanalysis can help people and seems to be pretty good for me too.
What do you consider your biggest challenge in becoming an analyst?
As I’ve come to discover, most of my “challenges” in any domain are my own doing. I seem to have some resistances left to resolve.
How has it changed your work (and yourself)?
I wish for my answer to convey confidence, not arrogance. Truthfully, the work has just gotten easier and a lot more fun. I don’t have to have the answers. I do have to know myself and be open enough to share parts of myself with my patients. As I’ve developed my ability to more freely communicate with patients, I believe it is carrying over into my personal life – well at least moving in that direction. After all, I am a work in progress.
Would you recommend institute training and why?
On this, I can only offer a qualified response. I absolutely would advise anyone serious about being a competent and helpful therapist to engage in some form of advanced post-graduate training – A degree, license, and CEUs are not enough. Based on my experiences as a student and now as an instructor, I wholeheartedly recommend IPS for people who are curious, open, and nice. That said, psychoanalysis is not for every patient and it’s not for every clinician. Fortunately, there are other differently-oriented post-graduate training programs that enroll curious, open, and nice people too.
Do you have a specialty or preferred population and why?
I do enjoy testing and therapy with the nice people of all ages, but I think I derive a greater sense of satisfaction working with challenging patients. I love seeing the movement that helps those people with serious problems let go of destructive fantasies and the drives to act on primitive impulses.
How do you spend your leisure time when not in the consulting room?
Aside from time spent with family, cooking, theater, and reading, most of the rest of my time outside of the consulting room, leisure or otherwise, is spent commuting and procrastinating. I’m still working to cultivate my ability to be leisurely
Tom Grace
Graduate of IPS and Faculty Member
|
|
METAPHORS BE WITH YOU
By Bill Goldberg
The Newsletter editors and our spouses recently traveled to the Galapagos Islands where we learned some fascinating facts about evolution and adaptability.
The phrase Survival of the Fittest is usually attributed to Charles Darwin, although it was originally suggested by Herbert Spencer. Spencer and Darwin did not use the term
fit
in the sense of physically strong, but in the sense of being able to evolve to fit the immediate local environment. Perhaps a more accurate way of phrasing the idea is
Survival of the Most Adaptable.
It can be difficult for our patients to change their perspective and their way of relating to the world even when their old ways are no longer working for them. In analysis, we try to provide our patients with room to adapt and to grow while acknowledging the fact that even positive growth and change can be discomforting. If we try to help them to free themselves to try a different response to a situation, or to adapt to stage of life changes, they may find accepting those changes to be less difficult if they can frame those changes as healthy adaptability
|
|
Bill Goldberg is now facilitating a group for clinicians who would like to write an article for publication. The purpose of the group is to help the participants overcome resistances and writers’ block with the help and support of colleagues who also are dealing with issues. Subjects that are covered include choosing a topic, researching the literature, formatting/editing the article, and deciding where to submit the it. Anyone interested in joining the group should contact Bill.
Lorna Goldberg has written a chapter entitled, “T
herapy with Former Members of Destructive Groups,
” for a book,
New Religious Movements and Counseling (2018), edited by Sarah Harvey, Silke Steidinger and James A. Beckford, published by
Routledge,
London and New York
.
School-Based Solutions to the Mental Health Crisis
On March 15, 2018, Zachary Schwartz, MSW, LCSW, PsyA conducted a webinar which was viewed by over 250 school professionals. Zack noted the complex and growing need for readily available child and adolescent mental health treatment. He pointed out that school-based professionals have noted a rise in anxiety, depression, school refusal, suicide and other mental health issues. Parents, teachers and community stakeholders expect the school professionals to address these mental health issues in the school environment The purpose of the webinar was to provide clarity for understanding how to respond and integrate mental health services in a school setting.
Zack discussed many topics, including the following:
· How school-based mental health over the past 100 years impacts the current school system
· The difference between traditional school-based counseling and intensive school-based counselling
· How to negotiate the expectations of school-based mental health needs to ensure that school professionals and parents/guardians work together
· Strategies for implementing a comprehensive school0based counseling program with existing school resources
· How to collect and use data to highlight the benefits and justify the appropriate level of mental health services in a school setting.
|
|
|
|
|
|
|