Infusion services and other therapies must be delivered without delay
by Erica R. Cohen, MD
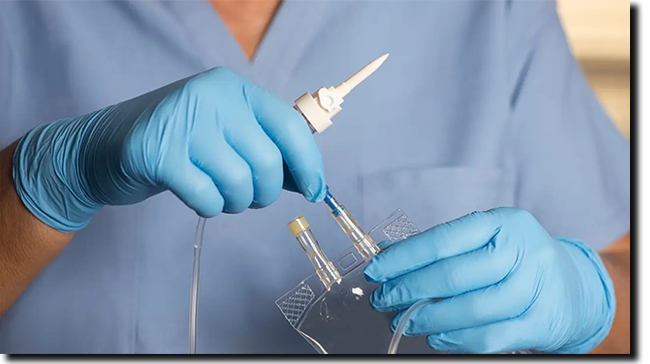
I often hear my patients ask the same questions: Why do I need to change to another infusible biosimilar again? Why do I need to get my infusion therapy sent by a specialty pharmacy? Will I be able to continue my therapy on time?
The answers are not straightforward. The story begins in 2016 when the first biosimilar came to market in the U.S. Biosimilars are near identical copies of the original therapy with the same active ingredient, mechanism of action, and risks -- but they cost less. They are made to be interchangeable with the original therapy. While this sounds reasonable at face value, the issue stems from onerous requirements implemented by insurance companies and pharmacy benefit managers (PBMs) mandating use of very specific "preferred" therapies. I've seen the consequences firsthand at my community practice that provides infusion services.
My patient Savannah* is a classic example. She has ulcerative colitis, a chronic condition that causes inflammation in her colon. It took quite a bit of time until we found her the appropriate infusion therapy and dosing schedule to get her into remission and feeling well. Savannah's insurer subsequently required her to change to another biosimilar. However, the required prior authorization was repeatedly denied, which delayed her therapy and risked disease recurrence.
Read More
| |
The text of the final health workplace safety standard has not been made public, though, leaving advocates in the dark about the details.
Lobbyists representing hospitals, nursing homes, retail pharmacies, and construction companies are pushing back on the Biden administration’s plans to finalize COVID-19 protections for workers in health care settings, arguing it would be unnecessary and burdensome in a still uncertain time.
It’s a fight that may spark a legal battle with the Occupational Safety and Health Administration over the rule, which aims to make permanent the emergency safety standards for health workplaces enacted in 2021.
The temporary rule, which OSHA stopped enforcing last year, included requirements surrounding ventilation, protective equipment and COVID testing and vaccination mandates, among other things. In finalizing it, the agency is considering whether to broaden the requirements and extend them to additional sectors such as construction workers inside a hospital. The rule will reportedly not, however, include a vaccine mandate.
Read More
| |
Increase corresponds to a climb in Medicare Advantage enrollment
Use of prior authorization in the Medicare Advantage (MA) program continues to increase, according to a report from KFF.
More than 46 million prior authorization requests were submitted to Medicare Advantage insurers on behalf of Medicare Advantage enrollees in 2022, up from 37 million in 2019, the report found. However, the average number of requests per enrollee was 1.7, the same as in 2019. "The rise in the total number of prior authorization requests corresponded to increasing enrollment in Medicare Advantage and so translated into a similar number of requests per enrollee," wrote report authors Jeannie Fuglesten Biniek, Nolan Sroczynski, and Tricia Neuman, all of KFF's Center on Medicare Policy.
Of the requests submitted, 90.4% were approved in full, while 7.4% were denied -- an increase from 5.7% in 2019, according to the report. And of those that were denied, about 10% were appealed, and of those, 83% resulted in the denial being overturned.
Read More
| |
Brain markers of degeneration, injury were better, too
An anti-inflammatory diet was tied to a lower risk for dementia in people ages 60 and older with cardiometabolic diseases, U.K. Biobank data showed.
Among people with cardiometabolic diseases including type 2 diabetes, heart disease, or stroke, those who were on an anti-inflammatory diet had a 31% lower risk for dementia compared with those on a pro-inflammatory diet (HR 0.69, 95% CI 0.55-0.88, P=0.003), reported Abigail Dove, MSc, of the Aging Research Center at the Karolinska Institute in Stockholm, and co-authors.
In a joint effect analysis, the hazard ratio for dementia among people with cardiometabolic disease was 1.65 (95% CI 1.36-2.00) with an anti-inflammatory diet, 1.91 (95% CI 1.57-2.32) with a neutral diet, and 2.38 (95% CI 1.93-2.93) with a pro-inflammatory diet over 12 years of follow-up.
Read More
| |
|
Patients with psoriasis, uveitis, or colitis who present with undiagnosed chronic back pain should be referred to a rheumatologist for the assessment of axial spondyloarthritis (axSpA), with MRI being a more accurate diagnostic method than clinical features.
METHODOLOGY:
- Researchers assessed the prevalence of axSpA according to the extra-articular presentation and human leukocyte antigen B27 (HLA-B27) status in two Canadian cohorts (SASPIC 1 and 2).
- Overall, 363 adult patients aged ≤ 45 years with psoriasis, uveitis, or colitis who presented with chronic undiagnosed back and/or buttock pain lasting 3 months or more were included.
- Participants were referred to rheumatologists with expertise in axSpA for structured diagnostic evaluations, including history, physical exam, levels of C-reactive protein, HLA-B27 status, and imaging studies.
Read More
| |
|
Virtual
August 31 & September 28
Click here for the complete list of upcoming exams.
ABIPP Part I; ABIPP Path - Combined DCCPM/CSM virtual exam;
ABIPP Competency Exam in IPM; ABIPP Competency Exam in Regenerative Medicine;
CSM Competency Exam; DCCPM Competency Exam
In Person
October 18, 2024
ABIPP Part II - Practical Examination
Lab Venue: MERI, 44 S. Cleveland Street, Memphis, TN 38104
| |
Faulty testing protocols threaten the freedom of those entangled in the U.S. legal system
When Anthony Bing called his doctor's office, it wasn't for a new symptom or a prescription refill. Instead, the 64-year-old man was worried about going to jail.
As part of his probation requirements, he was subject to urine testing twice a week at a Philadelphia probation office. Those tests had come back positive for alcohol five times in a row, according to Bing's physician. Now his probation and his freedom were in jeopardy.
There was just one problem: The Navy veteran had not had a drop of alcohol in almost a year. But the test said otherwise. How could he find out what went wrong in time to stop the court from sending him behind bars?
Read More
| |
Registration is open for
ASIPP's 2025 Annual Meeting
We would love it if you would register and join us in Orlando!
| |
|
A surprising therapy is showing promise for chronic pain, vision loss, and muscle recovery, among other conditions.
It's not a pill, an injection, or surgery. It's light. Yes, light. The thing that appears when you open the curtains, flip a switch, or strike a match.
Light illuminates our world and helps us see. Early human trials suggest it may help us heal in new ways as well.
"Phototherapy is still in its infancy," said Mohab Ibrahim, MD, PhD, a professor of anesthesiology at the University of Arizona, Tucson, Arizona, who studies the effects of light on chronic pain. "There are so many questions, a lot of things we do not understand yet. But that's where it gets interesting. What we can conclude is that different colors of light can influence different biological functions."
Read More
| |
ASIPP State Society Meeting: | |
|
What if a drug could help you live a longer, healthier life?
Scientists at the University of Connecticut are working on it. In a new study in Cell Metabolism, researchers described how to target specific cells to extend the lifespan and improve the health of mice late in life.
The study builds on a growing body of research, mostly in animals, testing interventions to slow aging and prolong health span, the length of time that one is not just alive but also healthy.
"Aging is the most important risk factor for every disease that we deal with in adult human beings," said cardiologist Douglas Vaughan, MD, director of the Potocsnak Longevity Institute at Northwestern's Feinberg School of Medicine, Chicago. (Vaughan was not involved in the new study.) "So the big hypothesis is: If we could slow down aging just a little bit, we can push back the onset of disease."
Read More
| |
- ASIPP Members Only Site Information - | |
-
To log in for the first time you will need to click “forgot password” at the bottom of the login window.
- Check your email and then log in as directed.
-
If you have problems logging into your account, click here.
| |
|
Pain Medicine Case Reports (PMCR) and Editor-in-Chief Alaa Abd-Elsayed, MD, PhD would like to invite you to submit case reports and case series to the PMCR journal. Your article will be published free of charge.
Open access journals are freely available online for immediate worldwide open access to the full text of published articles. There is no subscription fee for open access journals. Open access journals are no different from traditional subscription-based journals: they undergo the same peer review and quality control as any other scholarly journal.
Interested in becoming a member of the PMCR Editorial Board?
Editorial board members are asked to review 2-6 manuscripts per year. Please submit your most up-to-date CV to sgold@asipp.org for consideration.
For more information or to submit your articles, click here.
| |
|
Christian Nicolosi, MD, Christina Draganich, DO, and George Marzloff, MD
Abstract
BACKGROUND: Neuropathic pain is a common, but difficult-to-treat, condition affecting the quality of life of many. It is prevalent in patients with multiple sclerosis (MS), an autoimmune chronic inflammatory disease of the central nervous system. Treatments, such as gabapentin, pregabalin, tricyclic antidepressants, serotonin, and norepinephrine reuptake inhibitors, are insufficient. As a result, botulinum neurotoxin type A (BoNT-A) has been explored for its effects on pain control with neuropathic pain.
CASE REPORT: We present a 59-year-old woman with chronic neuropathic pain and MS. She presented to us with allodynia in the lateral portion of her left trunk, radiating into her breast to the nipple. The patient reported improvement in pain after subcutaneous injections of BoNT-A over the area of pain.
CONCLUSIONS: In the present case report, we highlight the effectiveness of subcutaneous BoNT-A for the treatment of refractory central neuropathic pain in MS.
KEY WORDS: Botulinum toxin type-A, central neuropathic pain, multiple sclerosis, subcutaneous injections, at-level pain
Read More
| |
New!
Updated Antithrombotic Guidelines now available!
| |
|
Laxmaiah Manchikanti, MD, Mahendra R. Sanapati, MD, Devi Nampiaparampil, MD, Byron J. Schneider, MD, Alexander Bautista, MD, Alan D. Kaye, MD, PhD, Nebojsa Nick Knezevic, MD, PhD, Alaa Abd-Elsayed, MD, Annu Navani, MD, Paul J. Christo, MD, Standiford Helm II, MD, Adam M. Kaye, PharmD, Jay Karri, MD, Vidyasagar Pampati, MSc, Sanjeeva Gupta, MD, Vivekanand A. Manocha, MD, Amol Soin, MD, Mayank Gupta, MD, Sanjay Bakshi, MD, Christopher G. Gharibo, MD, Kenneth D. Candido, MD, Anjum Bux, MD, Anilkumar Vinayakan, MD, Vinayak Belamkar, MD, Scott Stayner, MD, PhD, Sairam Atluri, MD, Sara E. Nashi, MD, Megan K. Applewhite, MD, Chelsi Flanagan, DO, Emiliya Rakhamimova, BA, Gerard Limerick, MD, PhD, Kunj G. Patel, MD, Sierra Willeford, DO, and Joshua A. Hirsch, MD
Abstract
BACKGROUND: The frequency of performance of interventional techniques in chronic pain patients receiving anticoagulant and antiplatelet therapy continues to increase. Understanding the importance of continuing chronic anticoagulant therapy, the need for interventional techniques, and determining the duration and discontinuation or temporary suspension of anticoagulation is crucial to avoiding devastating complications, primarily when neuraxial procedures are performed. Anticoagulants and antiplatelets target the clotting system, increasing the bleeding risk. However, discontinuation of anticoagulant or antiplatelet drugs exposes patients to thrombosis risk, which can lead to significant morbidity and mortality, especially in those with coronary artery or cerebrovascular disease. These guidelines summarize the current peer reviewed literature and develop consensus-based guidelines based on the best evidence synthesis for patients receiving anticoagulant and antiplatelet therapy during interventional procedures.
STUDY DESIGN: Review of the literature and development of guidelines based on best evidence synthesis.
OBJECTIVES: To provide a current and concise appraisal of the literature regarding the assessment of bleeding and thrombosis risk during interventional techniques for patients taking anticoagulant and/or antiplatelet medications.
METHODS: Development of consensus guidelines based on best evidence synthesis included review of the literature on bleeding risks during interventional pain procedures, practice patterns, and perioperative management of anticoagulant and antiplatelet therapy. A multidisciplinary panel of experts developed methodology, risk stratification based on best evidence synthesis, and management of anticoagulant and antiplatelet therapy. It also included risk of cessation of anticoagulant and antiplatelet therapy based on a multitude of factors. Multiple data sources on bleeding risk, practice patterns, risk of thrombosis, and perioperative management of anticoagulant and antiplatelet therapy were identified. The relevant literature was identified through searches of multiple databases from 1966 through 2023.
In the development of consensus statements and guidelines, we used a modified Delphi technique, which has been described to minimize bias related to group interactions. Panelists without a primary conflict of interest voted on approving specific guideline statements. Each panelist could suggest edits to the guideline statement wording and could suggest additional qualifying remarks or comments as to the implementation of the guideline in clinical practice to achieve consensus and for inclusion in the final guidelines, each guideline statement required at least 80% agreement among eligible panel members without primary conflict of interest.
RESULTS: A total of 34 authors participated in the development of these guidelines. Of these, 29 participated in the voting process. A total of 20 recommendations were developed. Overall, 100% acceptance was obtained for 16 of 20 items. Total items were reduced to 18 with second and third round voting. The final results were 100% acceptance for 16 items (89%). There was disagreement for 2 statements (statements 6 and 7) and recommendations by 3 authors. These remaining 2 items had an acceptance of 94% and 89%. The disagreement and dissent were by Byron J. Schneider, MD, with recommendation that all transforaminals be classified into low risk, whereas Sanjeeva Gupta, MD, desired all transforaminals to be in intermediate risk. The second disagreement was related to Vivekanand A. Manocha, MD, recommending that cervical and thoracic transforaminal to be high risk procedures.
Thus, with appropriate literature review, consensus-based statements were developed for the perioperative management of patients receiving anticoagulants and antiplatelets These included the following: estimation of the thromboembolic risk, estimation of bleeding risk, and determination of the timing of restarting of anticoagulant or antiplatelet therapy.
Risk stratification was provided classifying the interventional techniques into three categories of low risk, moderate or intermediate risk, and high risk. Further, on multiple occasions in low risk and moderate or intermediate risk categories, recommendations were provided against cessation of anticoagulant or antiplatelet therapy.
LIMITATIONS: The continued paucity of literature with discordant recommendations.
CONCLUSION: Based on the review of available literature, published clinical guidelines, and recommendations, a multidisciplinary panel of experts presented guidelines in managing interventional techniques in patients on anticoagulant or antiplatelet therapy in the perioperative period. These guidelines provide a comprehensive assessment of classification of risk, appropriate recommendations, and recommendations based on the best available evidence.
KEY WORDS: Perioperative bleeding, bleeding risk, practice patterns, anticoagulant therapy, antiplatelet therapy, interventional techniques, safety precautions, pain
DISCLAIMER: These guidelines are crafted from the most up-to-date evidence and are not intended as rigid treatment mandates. Given the evolving nature of scientific evidence, this document does not aim to establish a definitive “standard of care.”
Read More
| |
|
Laxmaiah Manchikanti, MD, Mahendra R. Sanapati, MD, Vidyasagar Pampati, MSc, Amol Soin, MD, and Joshua A. Hirsch, MD
Abstract
BACKGROUND: The role of antiplatelet/anticoagulant therapy is well known for its primary and secondary prevention of sequela from cardiovascular disease by decreasing the incidence of acute cerebral, cardiovascular, peripheral vascular, and other thrombo-embolicevents. The overwhelming data show that the risk of thrombotic events is significantly higher than that of bleeding during surgery after antiplatelet drug discontinuation. It has been assumed that discontinuing antiplatelet therapy prior to performing interventional pain management techniques is a common practice, even though doing so may potentially increase the risk of acute cerebral and cardiovascular events.
A survey of practice patterns was conducted in 2012, since then the risks associated with thromboembolic events and bleeding, has not been systematically evaluated.
OBJECTIVE: To conduct an updated assessment of the perioperative antiplatelet and anticoagulant practice patterns of U.S. interventional pain management physicians and compare this with data collected in 2012 with 2021 data regarding practice patterns of continuing or discontinuing anticoagulant therapy.
STUDY DESIGN: Postal survey of interventional pain management physicians.
STUDY SETTING: Interventional pain management practices in the United States.
METHODS: The survey was conducted based on online responses of the members of the American Society of Interventional Pain Physicians (ASIPP) in 2021. The survey was designed similar to the 2012 survey to assess updated practice patterns.
RESULTS: The questionnaire was sent out to 1,700 members in October 2021. Out of these, 185 members completed the survey, while 105 were returned due to invalid addresses.
The results showed that 23% changed their practice patterns during the previous year. The results also showed that all physicians discontinued warfarin therapy with the majority of physicians accepting an INR of 1.5 as a safe level. Low dose aspirin (81 mg) was discontinued for 3 to 7 days for low-risk procedures by 8% of the physicians, 34% of the physicians for moderate or intermediate risk procedures, whereas they were discontinued by 76% of the physicians for high-risk procedures. High dose aspirin (325 mg) was discontinued at a higher rate. Antiplatelet agents, including dipyridamole, cilostazol, and Aggrenox (aspirin, extended-release dipyridamole) were discontinued from 3 to 5 days by 18%-23% of the physicians for low-risk procedures, approximately 60% of the physicians for moderate or intermediate-risk procedures, and over 90% of the physicians for high-risk procedures. Platelet aggregation inhibitors clopidogrel, prasugrel, ticlopidine, and ticagrelor were discontinued for 3 to 5 days by approximately 26% to 41% for low-risk procedures, almost 90% for moderate or intermediate-risk procedures, and over 97% for high-risk procedures. Thrombin inhibitor dabigatran was discontinued by 33% of the physicians for low-risk procedures, 92% for moderate or intermediate-risk procedures, and 99% for high-risk procedures. Anti-Xa agents, apixaban, rivaroxaban, and Edoxaban were discontinued in over 25% of the physicians for low-risk procedures, approximately 90% for moderate or intermediate-risk procedures, and 99% for high-risk procedures.
LIMITATIONS: This study was limited by its being an online survey of the membership of one organization in one country, that there was only a 11.6% response rate, and the sample size is relatively small. Underreporting in surveys is common. Further, the incidence of thromboembolic events or epidural hematomas was not assessed.
CONCLUSION: The results in the 2021 survey illustrate a continued pattern of discontinuing antiplatelet and anticoagulant therapy in the perioperative period. The majority of discontinuation patterns appear to fall within guidelines.
KEY WORDS: Interventional pain management, interventional techniques, hemostasis, anticoagulants, antiplatelet therapy, thromboembolic events, bleeding, complications, aspirin, clopidogrel (Plavix), warfarin (Coumadin).
Read More
| |
|
ASIPP is now in collaboration with Curi Medical Liability Program
| |
|
Since this malpractice insurance program officially launched in November 2018, ASIPP has signed up hundreds of providers with an average savings of 30%. This is professional liability insurance tailored to our specialty and will stand up for us and defend our practices.
Curi is a full-service advisory firm that serves physicians and their practices. Their valued advice is grounded in your priorities and elevated in your outcomes. They are driven by a deep understanding of your specific circumstances in medicine, business, and life. To read a few important points to keep in mind about the program, including discounts, administrative defense, cyber coverage, aggressive claims handling, and complimentary risk management CME activities, visit our website.
| | |
|
Group Purchasing Organization Offer Better Pricing and Creates Added Value
ASIPP has formed a partnership with Henry Schein and PedsPal, a national GPO that has a successful history of negotiating better prices on medical supplies and creating value-added services for independent physicians. Working with MedAssets, PedsPal provides excellent pricing on products like contrast media that alleviate some of the financial pressures you experience today.
Learn More
| |  |
|
ASIPP, Fedora Billing,
and Revenue Cycle Management Partnership
ASIPP is now offering our members the benefit of a unique revenue cycle management/ billing service.
We have received a tremendous amount of interest in the ASIPP® billing and coding program.
Click here to learn more about the negotiated rate for practices and more!
| |
|
Like and follow ASIPP® on Facebook, X, and LinkedIn for the most
up-to-date news related to you, your practice, and your patients!
| | | | |