|
Join ASIPP’s VoterVoice Campaign:
Fight Medicare Physician Payment Cuts!
ASIPP Members, Interventional Pain Physicians, and patients, we need your active participation to protect patients’ access to care! CMS has revealed the 2024 Physician Fee Schedule, and it brings ominous news. You can help preserve our patients’ access to care by promptly signing the sample letters below.
Physicians, click here to use VoterVoice to send a letter to your representatives online, or use this sample letter to send on your own. Get your patients involved by asking them to sign this letter, and then have them, or your staff, enter the letter into VoterVoice by clicking here.
| |
|
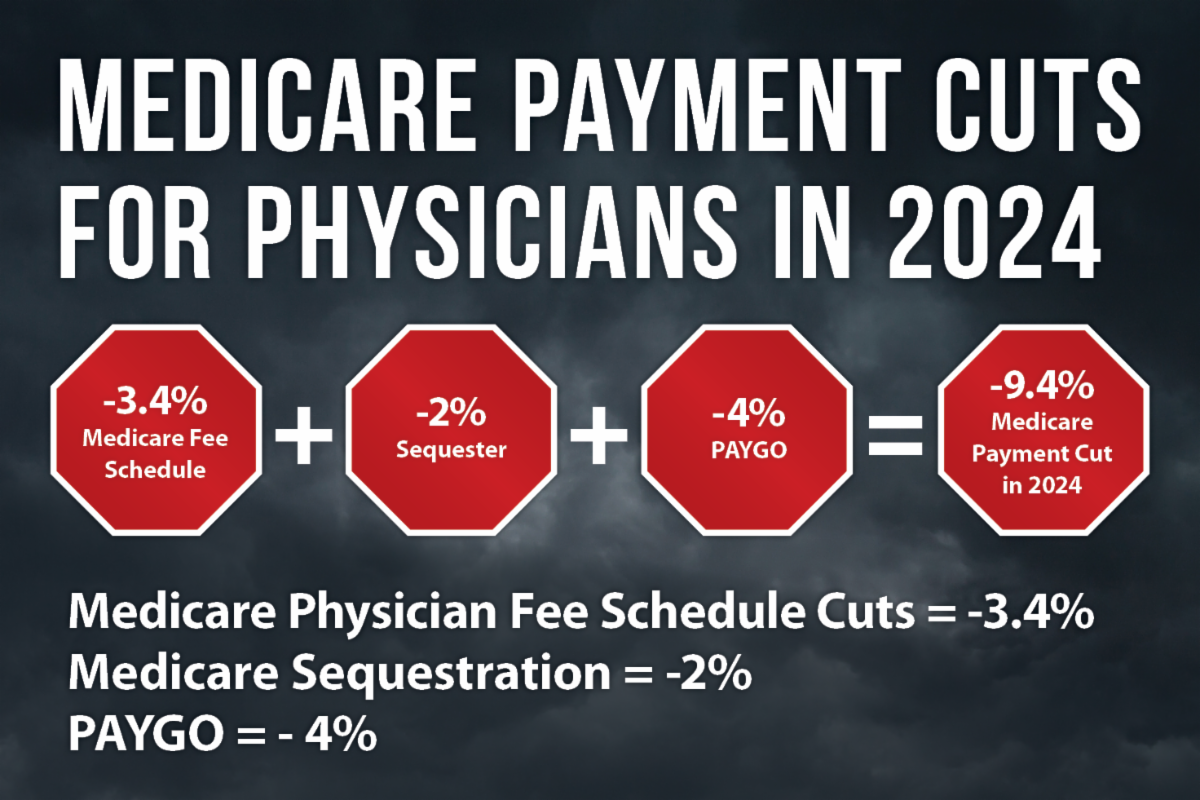
CMS has published the final rule for 2024 Physician Fee Schedule
The final Medicare payment cuts include:
Medicare Physician Fee Schedule Cuts = -3.4%
- The Centers for Medicare and Medicaid Services are implementing a 3.4% decrease in payments in 2024 for services under the Medicare Physician Fee Schedule.
-
Medicare physician payment has been reduced 26% adjusted for inflation from 2001–2023.
Medicare Sequestration= -2%
- Medicare sequestration of -2% has now been extended through 2032, because of a temporary delay for 1½ years.
There is some good news. The 4% PAYGO cut is gone for this year. It will reappear next year.
ASIPP members in good standing can access the physician, ASC, and HOPD fee schedule, on the Members’ Only Website.
How you can take action:
-
VoterVoice: Click here to submit a physician letter online!
-
VoterVoice: Click here to submit a patient letter online!
-
If you choose to send your own letters, here is sample physician letter you may want to use: PHYSICIAN SAMPLE LETTER.
-
Ask your patients to sign this sample patient letter. Your patients or your staff can enter the letter into VoterVoice: PATIENT SAMPLE LETTER.
| |
Early Bird Registration is open for ASIPP Members!
Register now for 10% off!
| |
|
Nobel Winner Drew Weissman Shares 7 Insights On Future mRNA Breakthroughs
If you, like me, are among the several billion people who received an mRNA Covid-19 vaccine, we have benefited from one of the greatest medical breakthroughs in human history. And we have many scientists to thank, including American physician and immunologist Drew Weissman, who shared this year’s Nobel Prize in Physiology or Medicine with his research partner Katalin Karikó. Last week, I had the honor of speaking to Weissman about how he envisions the future of mRNA vaccines and therapies.
For quick background, Weissman and Karikó spent years solving the incredibly complex problem of how to dampen the harmful effect of lab-made mRNAs on the immune system. In a landmark paper in 2005 in the journal Immunity, they reported that a substitution of one chemical base of the mRNA molecule for another modified base nearly eliminated the immune reaction. Several of their later papers showed that the modified mRNA also greatly increased protein production compared to unmodified mRNA.
Their breakthrough helped lay the foundation for the Covid-19 vaccines, which cleverly train our bodies to prepare to fight the virus without seeing the real thing. As the Nobel Assembly wrote in its announcement of this year’s award, “Through their groundbreaking findings, which have fundamentally changed our understanding of how mRNA interacts with our immune system, the laureates contributed to the unprecedented rate of vaccine development during one of the greatest threats to human health in modern times.”
Read More
| |
|
Virtual
December 9 & 16, 2023
ABIPP Part I; ABIPP Path - Combined DCCPM/CSM virtual exam;
ABIPP Competency Exam in IPM; ABIPP Competency Exam in Regenerative Medicine
January 20, 2024
ABIPP Part I; ABIPP Path - Combined DCCPM/CSM virtual exam;
ABIPP Competency Exam in IPM; ABIPP Competency Exam in Regenerative Medicine;
Controlled Substance Management (CSM) Competency Exam
February 17, 2024
ABIPP Part I; ABIPP Path - Combined DCCPM/CSM virtual exam;
ABIPP Competency Exam in IPM; ABIPP Competency Exam in Regenerative Medicine;
CSM Competency Exam; DCCPM Competency Exam
In-Person
June 21, 2024
ABIPP Part II Practical Examination
Lab Venue: Oquendo Center, 2425 E. Oquendo Rd, Las Vegas, NV 89109
| |
|
Seek and Ye Shall Find Afib in Stroke Survivors
Neuro-cardiac collaboration can make a big difference post-stroke
In 2023, stroke remains the fifth leading cause of death in the U.S. and a leading cause of long-term disability. After a stroke, the 5-year risk of myocardial infarction or vascular death is 17% and the 4-year risk of recurrent stroke is 18%.
As a vascular (stroke) neurologist, my role is to uncover the cause of the patient's stroke and begin the process of "risk factor modification" in order to prevent the next stroke from happening. Today, there are numerous causes of stroke (smoking, inactivity, hypertension), many of which are related to the heart. Of the strokes caused by heart issues, the leading cause is atrial fibrillation (Afib), which is associated with a fivefold increased stroke risk. Therefore, detecting Afib and creating a tailored care and monitoring plan is essential.
Eye on the Heart of Stroke Survivors
After a stroke, there's value in keeping a close eye on a patient and their heart. Integrating a full cardiac work-up while the stroke survivor is recovering in the hospital is the first step. This includes echocardiogram and electrocardiogram in the hospital with continuous telemetry monitoring during the entire admission. As discharge day approaches, we create a plan for ongoing outpatient cardiac monitoring for the long-term. Despite this thorough workup to try to find the cause, up to 30% of patients get diagnosed with cryptogenic stroke (unknown cause). Because every patient (and every stroke) is different, it is vital to build tailor-made, post-stroke cardiac risk-factor assessment strategies based on each patient's specific metrics, labs, and brain, neck, and heart imaging.
Read More
| |
|
Excellent opportunities for Residents & Fellows
at ASIPP's 2024 Annual Meeting:
-
Resident & Fellow Scholarship - Limited to 100!
- Abstract Session (April 4, 3:30-5:30pm) and Podium Presentation for Best Abstracts during General Session (April 5, 3:30-4:15pm)
- Half-Day Session dedicated to Young Physicians in Interventional Pain Management
| |
|
A Wake-Up Call for Physicians: Our Scope of Practice Includes the Climate
The Fifth National Climate Assessment recognizes the broad impact of the environment on health
As hospitalists, our scope of practice is rapidly expanding. No longer can we be content addressing the chief complaint and the symptoms at admission. No longer can we even just focus on barriers to care and issues of inequity as the social determinants of health. The stealth advance of the climate crisis threatens the health of all our patients. In the face of environmental degradation, we must address ecological determinants of health, which extend far beyond our traditional medical training.
This week marks the release of the Fifth National Climate Assessment (NCA). Broad in scope and sophisticated in its analysis, this Congressionally mandated report is the most comprehensive federal analysis of climate change to date and serves to inform government policy at every level. In contrast to the last NCA released in 2018, the Fifth NCA is influenced by the social sciences and Indigenous studies. The report acknowledges that our fossil-fuel built society has been profoundly unjust, emphasizing the outsized impact on disadvantaged populations such as the poor, marginalized communities, and vulnerable populations like pregnant women, children, and the elderly.
Physicians need to recognize that this report is not just about the ice caps melting. The climate crisis directly affects patient care. Extreme heat leads not only to heat stroke but also to renal disease, adverse pregnancy outcomes, cardiovascular and respiratory diseases, and mental health impacts, with heat-related illness and death projected to increase without drastic steps toward adaptation and mitigation. Wildfires have impacted large swaths of the U.S., leading to dangerously poor air quality; this affects reproductive health, cardiac and pulmonary disease, and influences changes in cognition and brain activity, exacerbating declines in well-being and mental health. This can also lead to conditions such as post-traumatic stress disorder, anxiety, depression, and suicide. As our ecology changes, we see shifts in vector-borne illnesses, amebic illnesses, and fungal disease. Pollution from fossil fuel combustion leads to lung adenocarcinoma while proximity to fracking sites increases rates of childhood leukemia.
Read More
| |
Abstract submissions are open for
ASIPP's 2024 Annual Meeting!
The submission deadline is January 22, 2024.
Don't miss your chance to be part of an exceptional event,
sharing insights and discoveries that shape the future of pain management.
| |
|
A Fourth of Med Students Want to Quit: The Humanities Can Help Them Reconnect
How a narrative approach can help trainees find joy in medicine
An alarming new report by Elsevier Health found that one in every four medical students in the U.S. has thought about quitting their studies. This is on top of the one in three physicians planning to reduce their work hours in the next 12 months and the one in five who plan to leave medicine altogether.
The Scope of the Problem
The Elsevier report includes more bad news. Over half of U.S. medical students plan to pursue healthcare careers that do not involve direct patient care. Globally, 60% of these students in healthcare are worried about their own mental health. This should concern not only those of us who teach or mentor medical students and residents; it should also concern anyone who wants to have a doctor in the next 10 years. The healthcare system is in crisis. According to Christine Sinsky, the American Medical Association vice president of professional satisfaction, "If even one-third to one-half of nurses and physicians carry out their expressed intentions to cut back or leave, we won't have enough staff to meet the needs of patients."
Other concerns cited by the more than 2,000 global healthcare students surveyed for the Elsevier study include financial pressures, work-life balance, the current pervasive culture of medical misinformation, as well as the shortages and burnout already being reported in our field. As a pediatrician, I am gravely concerned by these new statistics. As the writer-in-residence at a family medicine residency program leading narrative medicine workshops for residents, I think I have a solution.
Read More
| |
|
States Making Progress Toward Setting Payment Limits for Some Drugs
Prescription drug affordability boards are now the law in eight states
As drug prices continue to rise, some states are fighting back through the use of prescription drug affordability boards (PDABs), which usually set limits on how much some patients will have to pay for medications.
PDABs were the brainchild of Jennifer Reck and colleagues at the National Academy of State Health Policy (NASHP), which started working on the issue in 2016. "We were hearing from states that were really getting crushed by drug prices, and they needed the tools and resources to do something about them," Reck, who is project director of NASHP's Center for State Prescription Drug Pricing, said in a phone interview. "We convened a workgroup of state officials to dive into this topic, and the idea of a PDAB was one of the initial policy recommendations coming out of this."
Using Rate-Setting as a Tool
The idea behind the PDAB was that "rate-setting is something that's a common state activity, and looking to something like a public utility commission as an example, the state could create PDABs to review drug prices -- not to set prices, which would be a violation of federal law -- but instead to leverage the states' rate-setting authority to set upper payment limits (UPLs)," she explained. Importantly, the UPLs apply only to in-state transactions; anything broader would run afoul of the Commerce Clause in the U.S. Constitution, which bars one state from regulating what goes on in other states.
Read More
| |
- ASIPP Members Only Site Information - | |
-
To log in for the first time you will need to click “forgot password” at the bottom of the login window.
- Check your email and then log in as directed.
-
If you have problems logging into your account, click here.
| |
Pain Medicine Case Reports (PMCR) and Editor-in-Chief Alaa Abd-Elsayed, MD, PhD would like to invite you to submit case reports and case series to the PMCR journal. Your article will be published free of charge.
Open access journals are freely available online for immediate worldwide open access to the full text of published articles. There is no subscription fee for open access journals. Open access journals are no different from traditional subscription-based journals: they undergo the same peer-review and quality control as any other scholarly journal.
Interested in becoming a member of the PMCR Editorial Board?
Editorial board members are asked to review 2-6 manuscripts per year. Please submit your most up-to-date CV to sgold@asipp.org for consideration.
For more information or to submit your articles, click here.
| |
|
| CASE REPORT |
Spontaneous Thoracic Dural Tear Presenting With Postural Headache: A Case Report
Rebecca Greensapn, DO, Kevin Johnson, BA, Anil Chakravorty, BS, Terence Hillery, MD, and Chong Kim, MD
Abstract
BACKGROUND: Incidental dural tear (durotomy) is a known complication of many forms of spinal instrumentation. The majority of durotomy cases are due to a known traumatic force, such as an intentional durotomy during neuraxial anesthesia, or an unintentional tear during lumbar decompression surgery. However, spontaneous dural tears have occasionally been reported.
CASE REPORT: We report a case of a 16-year-old woman with postural headaches who was found to have a spontaneous thoracic dural tear on magnetic resonance imaging. She underwent a successful fluoroscopic-guided epidural blood patch with resolution of symptoms.
CONCLUSION: This case highlights the importance of considering spontaneous dural tears as a possible cause of postural headaches.
KEY WORDS: Spontaneous dural tear, traumatic dural tear, idiopathic dural tear, durotomy, post-dural postural headache, epidural blood patch, headache, CSF leak, case report
Read More
| |
|
| SYSTEMATIC REVIEW |
Radiofrequency Ablation’s Effectiveness for Treating Abdominal and Thoracic Chronic Pain Syndromes: A Systematic Review of the Current Literature
Benjamin Vachirakorntong, BS, Eric Kawana, BS, Vladislav Pavlovich Zhitny, MD, Brian J. Mendelson, MD, Brandon Esenther, MD, Adam J. Goodman, MD, and Ryan T. Gualtier, MD
Abstract
BACKGROUND: Many patients suffer from abdominal and thoracic pain syndromes secondary to numerous underlying etiologies. Chronic abdominal and thoracic pain can be difficult to treat and often refractory to conservative management. In this systematic literature review, we evaluate the current literature to assess radiofrequency ablation’s (RFA) efficacy for treating these debilitating chronic pain conditions in the thoracic and abdominal regions.
OBJECTIVES: The objective of this study is to determine the pain relief efficacy of RFA on chronic thoracic and chronic abdominal disease states.
STUDY DESIGN: This study is a systematic literature review that uses the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) method to gather academic literature articles through a methodical approach. The numbers obtained from each academic manuscript were then used to calculate the percent efficacy of radiofrequency ablation on thoracic and abdominal pain relief.
METHODS: Articles from 1992 through 2022 were gathered using PRISMA guidelines. The search terms “Radiofrequency Ablation Thoracic Pain” and “Radiofrequency Ablation Abdominal Pain” were used to identify articles to include in our study. Our search yielded a total of 575 studies, 32 of which were included in our study. The articles were then categorized into pain causes. The efficacy of RFA for each qualitative study was then quantified. Risk of bias was also assessed for articles using the Cochran Risk of Bias tool, as well as a tool made by the National Institutes of Health.
RESULTS: The PRISMA search yielded a total of 32 articles used for our study, including 16 observational studies, one cohort study, 6 case reports, 6 case series, and 3 clinical trials. Twenty-five articles were labeled good quality and one article was labeled fair quality according to the risk of bias assessment tools. The studies examined RFA efficacy on chronic abdominal and chronic pain syndromes such as spinal lesions, postsurgical thoracic pain, abdominal cancers, and pancreatitis. Among these etiologies, RFA demonstrated notable efficacy in alleviating pain among patients with spinal osteoid osteomas or osteoblastomas, lung cancer, and pancreatic cancer. The modes of RFA used varied among the studies; they included monopolar RFA, bipolar RFA, pulsed RFA, and RFA at different temperatures. The average efficacy rate was 84% ranging from 55.8% - 100%. A total of 329 males and 291 females were included with ages ranging 4 to 90 years old.
LIMITATIONS: Limitations of this review include the RFA not being performed at the same nerve level to address the same pathology and the RFA not being performed for the same duration of time. Furthermore, the efficacy of RFA was evaluated via large case series and single cohort observational studies rather than control group observational studies and clinical trial studies.
CONCLUSION: A systematic review of the literature supports RFA as a viable option for managing abdominal and thoracic pain. Future randomized controlled trials are needed to investigate the efficacy of the various RFA modalities to ensure RFA is the source of pain relief as a large body of the current literature focuses only on observational studies.
KEY WORDS: Chronic pain management, radiofrequency ablation, chronic abdominal pain, chronic thoracic pain, pain measurement
Read More
| |
|
| SYSTEMATIC REVIEW|
Hemodynamic Influences of Remimazolam Versus Propofol During the Induction Period of General Anesthesia: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Xilin Peng, MM, Congqi Liu, MM, Yihao Zhu, MM, Ling Peng, MD, Xueguang Zhang, MM, Wei Wei, MD, and Tao Zhu, MD
Abstract
BACKGROUND: Remimazolam is a novel ultrashort-effect benzodiazepine. In 2020, the US Food and Drug Administration approved it for procedural sedation. Remimazolam is beneficial for consistent sedation and quick recovery in painless gastrointestinal endoscopy. Propofol is one of the most commonly used intravenous anesthetics in clinical practice. Recently, only a few studies have compared propofol with remimazolam for general anesthesia induction.
OBJECTIVES: The purpose of our systematic review and meta-analysis was to compare the hemodynamic effects of remimazolam and propofol during the induction of general anesthesia.
STUDY DESIGN: Systematic review and meta-analysis of randomized, controlled trials.
METHODS: The authors retrieved the PubMed, Embase, Cochrane Library, and Web of Science databases for studies published through September 30, 2022, which reported relevant prospective randomized controlled trials (RCTs) comparing remimazolam with propofol for general anesthesia.
The primary outcome was hemodynamic changes, including the absolute value of fluctuation of mean arterial pressure (delta MAP) and heart rate delta HR). The secondary outcomes were the following 2 indicators: the occurrence of total adverse events and the quality of recovery from general anesthesia at 24 hours postsurgery. RevMan 5.4.1 (The Nordic Cochrane Centre for The Cochrane Collaboration) and trial sequential analysis were used to execute the statistical analyses. The different domains of bias were judged by the Cochrane risk of the bias assessment tool.
RESULTS: The authors identified 189 papers in PubMed, Embase, Cochrane Library, and Web of Science. Eight articles with 964 patients were selected. The included studies had moderate quality. For primary outcomes, the lower delta HR (mean difference [MD] = -4.99; 95% CI, -7.97 to -2.00; I² = 41.6%; P = 0.001] and delta MAP (MD = -5.91; 95% CI. -8.57 to -3.24; I² = 0%; P < 0.0001) represent more stable hemodynamic characteristics in the remimazolam group. Regarding secondary outcomes, a considerably lower incidence of total adverse events was noted in the remimazolam group than that for the propofol group (odds ratio [OR] = 0.40; 95% CI, 0.28 to 0.58; I² = 63%; P < 0.00001). In comparison to the propofol group, remimazolam achieved an advantage score of quality of recovery -15 in 24 hours postsurgery (MD = 5.31, 95% CI, 1.51 to 9.12; I² = 87%; P = 0.006).
LIMITATION: Firstly, there are only a handful of published RCTs on the administration of remimazolam in general anesthesia. In addition, due to patient privacy, we could not extract individual patient data, therefore we could not combine and assess any variations in patient characteristics.
CONCLUSION: Evidence suggests that remimazolam has a lower hemodynamic effect during general anesthesia and fewer perioperative adverse effects after general anesthesia than propofol; however, which agent is superior regarding quality benefit in postoperative recovery based on the studies included here remains inconclusive. Additional RCTs with updated meta-analyses to enlarge the sample size and properly analyze the benefit-to-risk ratio to patients are needed to determine the evidence for such a relatively new medicine.
KEY WORDS: Remimazolam, propofol, general anesthesia, hemodynamic, adult
Read More
| |
|
ASIPP is now in collaboration with Curi Medical Liability Program
| |
|
Since this malpractice insurance program officially launched in November 2018, ASIPP has signed up hundreds of providers with an average savings of 30%. This is professional liability insurance tailored to our specialty and will stand up for us and defend our practices.
Curi is a full-service advisory firm that serves physicians and their practices. Their valued advice is grounded in your priorities and elevated in your outcomes. They are driven by a deep understanding of your specific circumstances in medicine, business, and life. To read a few important points to keep in mind about the program, including discounts, administrative defense, cyber coverage, aggressive claims handling, and complimentary risk management CME activities, visit our website.
| | |
|
Group Purchasing Organization Offer Better Pricing and Creates Added Value
ASIPP has formed a partnership with Henry Schein and PedsPal, a national GPO that has a successful history of negotiating better prices on medical supplies and creating value-added services for independent physicians. Working with MedAssets, PedsPal provides excellent pricing on products like contrast media that alleviate some of the financial pressures you experience today.
Learn More
| |  |
|
ASIPP, Fedora Billing,
and Revenue Cycle Management Partnership
ASIPP is now offering our members the benefit of a unique revenue cycle management/ billing service.
We have received a tremendous amount of interest in the ASIPP® billing and coding program.
Click here to learn more about the negotiated rate for practices and more!
| |
|
Like and follow ASIPP® on Facebook, X, and LinkedIn for the most
up-to-date news related to you, your practice, and your patients!
| | | | |