|
DCJS Victims Services News | |
Sexual Assault Awareness Month
Special Edition
| |
|
|
Sexual Assault Awareness Month – April 2023
Chad Felts, Intimate Partner Gun Violence Prevention Coordinator
April 2023 marks the official 22nd anniversary of Sexual Assault Awareness Month (SAAM). This nationwide recognition was first organized and coordinated by the National Sexual Violence Resource Center (NSVRC). Established in July 2000, NSVRC acted quickly to survey local and regional sexual violence coalitions, leading to the formal establishment of SAAM in April 2001.
During the early 2000s, the primary goal of SAAM was increasing awareness of sexual assault, including both victims and survivors. As SAAM continued to grow, NSVRC began to incorporate prevention more heavily into its annual outreach efforts, targeting communities, college campuses, and workplaces. These campaigns focused on ways that individuals, communities, and advocacy groups can stop sexual assault before it occurs, by acknowledging warning signs and working to change behaviors.
NSVRC selects a new theme every April in an effort to highlight an emerging trend or topic. However, each year’s theme continues to advance several common goals: enhancing awareness of sexual assault nationwide, and increasing prevention through education about healthy sexuality, consent, and bystander intervention. As always, the teal ribbon, first selected by NSVRC in 2001, remains a powerful symbol, both for sexual assault awareness in general, and for the annual recognition that occurs each April.
The theme for 2023, Drawing Connections: Prevention Demands Equity, will address the challenges and hurdles faced by people of color in seeking out sexual assault services. SAAM 2023 calls on all individuals, communities, organizations, and institutions to challenge themselves and one another, in order to build and enhance racial equity and respect amongst sexual assault service providers and victims.
NSVRC – SAAM information and events
|  | |
Sexual Violence in Virginia:
Victim Profiles
Virginia State Police, Crime in Virginia, 2020 (2021)
82% of forcible sex offenses reported in 2020 were committed by perpetrators known by or acquainted with the victim.
37% of the reported forcible sex offenses were committed against family members or intimate dating partners.
52% of the forcible rapes reported to law enforcement agencies in 2020 were committed against male and female victims under the age of 18.
76% of forcible sex offenses reported to law enforcement agencies in 2020 occurred in a residence or home.
77% of victims who sought crisis services for an incident within 30 days of the incident reported it to law enforcement in Virginia.
|
|  |
Sexual Assault Awareness Month RESOURCES | |
Sexual Assault Awareness Month Video
Learn more about the prevalence of sexual assault and the impact sexual violence has on victims' lives.
| |
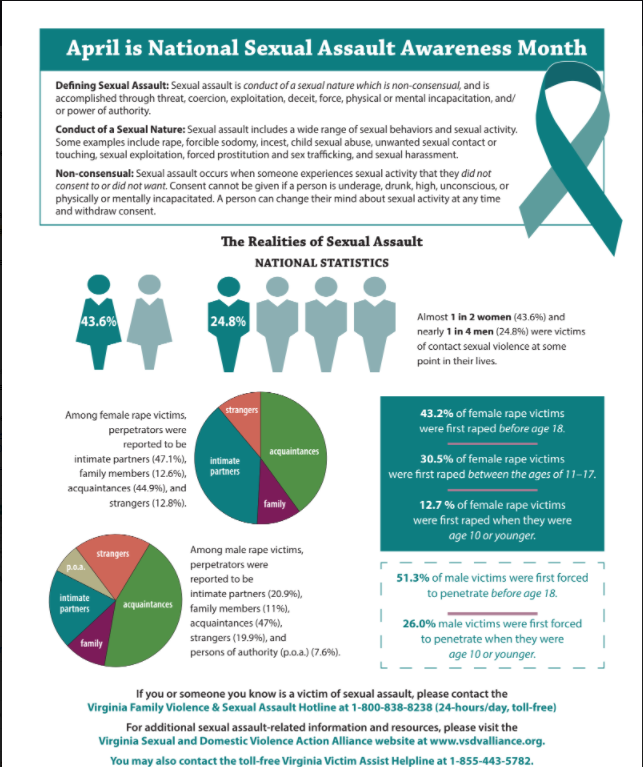
Sexual Assault Infographic Fact Sheet
This downloadable fact sheet contains statistics and resources related to sexual assault.
|
|
The Calm in the Storm: Resilience in the Face of Sexual Assault –
An Interview with
Ava Stokes
Andrea Sutton,
Sexual and Domestic Violence Program Professional Standards Consultant
April is Sexual Assault Awareness Month, and many survivors have a remarkable story to tell. This month we invited Ava Stokes to share her account of her sexual assault encounter.
The interview contains content that may be upsetting or traumatic, so please listen with caution.
If you are not able to listen to the interview but want to know what occurred here are some articles Ava wanted to share.
"Guilty verdict brings six consecutive life sentences"
"She's on their side: Survivor of Georgetown rape takes step toward victim advocacy goal"
"Georgetown rape survivor flooded with support from other survivors after telling her story"
| | |
|
“The Age of Overwhelm” – A Book Review
Bunny Chidester, Victims Services Program Specialist
Years ago, when I was working as a domestic violence advocate and preventionist, Laura van Dernoot Lipsky was the keynote presenter at the Action Alliance Retreat. She had recently published her first book, Trauma Stewardship, which was her retreat topic. It was a powerful moment, listening to her speak to all of us who were doing daily crisis intervention work, and perhaps not recognizing the personal toll that dealing with ongoing trauma was having on us as individuals, on our relationships and families, and on our communities. I bought two books and gifted one to a close friend who was working at the Department of Social Services/Child Protective Services (DSS/CPS). It became an invaluable and needed daily resource for him that he still keeps on his desk.
Enter The Age of Overwhelm, van Dernoot Lipsky’s next book, released in 2018. This book has been as useful as the first, with a focus on ways to recognize overwhelm, manage stress, learn to slow down, develop coping skills, and it is peppered with her signature humor and sharing of pertinent cartoons.
From the introduction: “Individuals are overwhelmed. Families are overwhelmed. Workplaces, communities, and entire systems are overwhelmed.” She dedicates the book to “those who are operating in a state of overwhelm some or all of the time.” She challenges us to examine what is within our control, and if circumstances are not within our control, to ask “What can I do to mitigate harm?” (to self, others, etc.), and “What can I do that would be helpful?” (pausing, noticing, taking something in, finding a way through). As a part of this self-examination, she asks us to answer, “How do you feel affected by your work and your life?” and “What would your loved ones want me to know…what would they say it’s like to be in a relationship with you?”
The book explores what overwhelm looks and feels like, as it can be difficult to have or maintain an awareness of a state of overwhelm. It discusses causes of overwhelm and how to become more mindful of its impact. The effects of screen time and social media on our mental health are examined. She advocates assessing our use of technology and considering unplugging more often. The impact of the 24-hour news cycle on our collective state of overwhelm is notable. She says, “What’s transpiring in the world, as well as how we’re taking it all in, is where I see a lot of folks reach a tipping point.” She recognizes the following important point, “Those who may be the target of racism or xenophobia or any kind of current supremacy that would have one fearing for one’s safety, life, or the well-being of loved ones may not have the privilege to disengage entirely from their screens.”
She adds, “More than half of U.S. workers with paid leave don’t take all their paid time off, and those who do often obsessively check and respond to emails while out of the office”, followed by a conclusion that being overwhelmed in a professional context has been proven to decrease productivity and happiness no matter the profession.
The author puts forth the idea that the first step in addressing overwhelm is to focus on doing less of that which erodes us and more of that which sustains us. She challenges us to tend to our ability to focus – to be intentional about what we attend to, when, and how, as a possible road through overwhelm.
Some other important points from the book:
- Protect your morning- start by regulating your breathing, and set a specific intention for the day, avoiding grabbing your phone as your first daily act.
- Manage the amount and intensity of distractions, especially phone and internet.
- Nurture gratitude.
- Disconnect less (from others, your environment, yourself), be present more- practicing being present quiets the overwhelm.
- Engage your breath, be active, get quality sleep, go outside, spend time with animals.
She recommends making small changes over time, adding things as you go. One concrete skill from the book that can be utilized in any situation: “When feeling a tightening within, try to slowly exhale, drop your shoulders, relax your jaw, and take a moment to close and open your hands a few times. Such a small exercise can be done in the classroom, boardroom, on the phone, or in traffic.”
Other practical skills include simplifying where possible. Reduce the volume of decisions made daily which contribute to “decision fatigue”. Examples include packing lunch and laying out clothes the night before and creating helpful routines while remaining flexible. Hold outdoor “walking meetings”. Take breaks to step outside and look at the sky.
And finally, she addresses when to step away. We have control over if and how much to be involved, connected, or engaged. “If it’s a small break you need to keep on keeping on, give yourself time and space to Just. Do. Nothing. Step out for a minute.” She adds, “Say “no” to something. Clear your plate a bit. Then consider setting stricter parameters where you allocate your time going forward.” She rightly observes from many years of trauma work, “Too often we gain clarity only after a crisis or when we’ve hit an all-time low.”
This book provides many important skills to utilize when feeling overwhelmed. It is a timely message for all of us right now, with U.S. and world events, recovery from the pandemic, and ongoing individual and collective struggles. I would suggest watching the author’s Ted Talk at this link https://www.youtube.com/watch?v=uOzDGrcvmus, and especially reading this powerful letter written from Laura to all trauma workers/advocates during the pandemic regarding stress/overwhelm/and not giving up:
https://traumastewardship.com/wp-content/uploads/2021/02/New_Trauma_Stewardship_Letter_PDF_W_Website_.pdf
| | |
|
A Survivor-Centered Approach to Addressing
Reproductive Coercion
Jennifer Kline, Improving Criminal Justice Responses Program Coordinator
Reproductive coercion is one of the most under-recognized ways that offenders exert control over their partners. Reproductive coercion is behavior that a partner uses to maintain power and control in a relationship related to reproductive and sexual health and includes a range of behaviors that may involve pressure, threats, sabotage, or manipulation to control the outcome of a pregnancy. Some examples of ways that partners may engage in reproductive coercion include attempts to impregnate a partner against her wishes, controlling outcomes of a pregnancy, coercing a partner to have unprotected sex, and sabotaging birth control methods.[1] One in five women report experiencing reproductive coercion and one in seven experience active interference with contraception.[2] Women with a history of intimate partner violence have significantly higher rates of unintended pregnancies.[3] Black (52.9%) and multiracial women (42.9%) are disproportionately affected by reproductive coercion compared to White women (20.6%).[4]
Advocacy organizations should promote survivor-centered approaches to encourage healing to help survivors regain the control the offender took from them. Our role as advocates is to provide options and resources in a nonjudgmental, supportive, and trauma-informed way for survivors to make the choices that are right for them to regain control and start the healing process. How can sexual and domestic violence organizations better support and empower survivors of sexual and reproductive coercion?
- Provide on-going training for staff on reproductive coercion.
- Include reproductive coercion questions on client intake and screening tools.
- Consider reproductive coercion when safety planning, to include providing information on tamper-proof birth control options.
- Develop and nurture partnerships with reproductive healthcare and family planning providers, to include referral protocols and cross-training.
- Create educational brochures and pocket cards with resources to give to survivors on reproductive coercion.
- Include sexual and reproductive healthcare information available on site in both English and Spanish.
-
Include all reproductive coercion education, screening, and safety planning in written policies and protocols.
- Provide reproductive coercion awareness and education to your community.
- Hire a nurse. Overall healthcare is an important piece of client and staff well-being, and survivors may be more likely to open up to a nurse about their healthcare needs.
In addition, reproductive healthcare and family planning providers should also have procedures for screening and referring survivors to advocacy organizations. Overall, it is crucial for advocates and healthcare providers to work together to create a comprehensive approach to addressing sexual and reproductive coercion. By providing survivors with the support, resources, and empowerment they need, we can help them break free from the cycle of violence and regain control over their lives.
For more information go to this reproductive coercion toolkit developed by the Virginia Sexual and Domestic Violence Action Alliance.
[1] Chamberlain, L. & Levenson, R. A Guide for Obstetric and Gynecological Reproductive Health Care Settings. 2013
[2] Futures Without Violence. (n.d.) The facts on reproductive health and partner abuse. http://www.futureswithoutviolence.org/userfiles/file/Children_and_Families/Reproductive.
[3] Pallitto, C. C., Garcia-Moreno, C., Jansen, H., Heise, L., Ellsberg, M., and Watts, C. (2012). Intimate partner violence, abortion, and unintended pregnancy: Results from the WHO multi-country study on women’s health and domestic violence. Gynecology & Obstetrics, 120(1), 3-9. https://doi-org.proxy.library.vcu.edu/10.1016/j.ijgo.
2012.07.003.
[4] Grace, K.T. (2016). Caring for women experiencing reproductive coercion. Journal of Midwifery & Women’s Health, 61(1), 112-115. https://doi-org.proxy.library.vcu.edu/10.1111/jmwh.12369
| | | |
|
How Does Someone Heal?
Dione Bassett, Victims Services Program Specialist
We do not always have the answer, but a survivor will know what’s right for them and what is useful in helping manage the effects of victimization. Healing is a unique experience for everyone. Unfortunately, sometimes the individuals we serve don’t know what options are available. The book Embodied Healing: Survivor and Facilitator Voices from the Practice of Trauma-Sensitive Yoga, states “Both the yoga and the therapeutic worlds have sets of beliefs about how a client should heal from trauma, but in truth healing must be survivor-led.” Survivors need the freedom to make choices about what feels safe and helpful. For some survivors, their faith community provides safety and support. For others, it could be a yoga class or music therapy. For someone else, it could be boxing. No option is successful for everyone. As advocates, simply asking the survivor what brings them joy and comfort can have a profound impact.
There is a significant connection between trauma and its effects on the body. To quote Peter Levine, author of Waking the Tiger:Healing Trauma, “Until we understand that traumatic symptoms are physiological as well as psychological, we will be woefully inadequate in our attempts to help them heal.” Traditional approaches such as talk therapy and crisis intervention remain critical in services. However, research is showing that healing trauma must include the mind, body, and spirit. I will never forget what a trainer once said about traditional services, “It’s like sitting down at a restaurant and not seeing anything you want on the menu”. What options do we have available for survivors? What healing modalities are in the community? Have we connected with them for guidance? To collaborate?
Here are some ways that alternative healing approaches can be incorporated into your service model:
-
Community Referral – Basic referrals, Reciprocal referrals, Sponsored referrals
-
Community Collaboration – Contracting with providers, Co-hosting public events or workshops
-
In-House Expertise – Existing staff and volunteers have expertise, Building in-house expertise among staff, Hiring someone with expertise HolisticHealingSASPPaperFINAL.pdf (nnedv.org)
Lastly, many survivors experience some form of anxiety. The book Overcoming Trauma Through Yoga: Reclaiming Your Body states that “people who are scared all the time develop bodies that somehow protect against this anxiety.” A method for reducing the effects of anxiety is through effective breathing. If you would like to try a breathing activity, please find some options here and share with others: https://www.verywellmind.com/abdominal-breathing-2584115
Healing for a survivor could begin with one intentional breath. One different approach or option. One person willing to offer something that hasn’t been offered before that somehow creates healing for the survivor. By exploring multiple options and connecting with survivors, the possibilities are endless.
https://www.barnesandnoble.com/w/embodied-healing-jennifer-turner/1136528492
https://www.goodreads.com/en/book/show/384924
https://www.amazon.com/Overcoming-Trauma-through-Yoga-Reclaiming/dp/1556439695
https://www.rainn.org/news/healing-ptsd-not-linear
| | |
|
Site Visits, Risk Assessments, and Findings, Oh My: Why Does the Virginia Department of Criminal Justice Services (DCJS) Conduct Site Visits?
Chrissy Smith,Victims Services Program Specialist
Have you ever heard of the Code of Federal Regulations (2 C.F.R.) Uniform Guidance? 2 C.F.R Part 200 establishes administrative requirements, cost principles, and audit requirements for Federal awards to non-Federal entities. It requires State Administering Agencies (SAA), like DCJS, to evaluate and monitor subgrantees to ensure compliance with federal and state regulations. DCJS developed risk-based policies and procedures for grant monitoring. Grant monitors conduct site visits based on this policy and procedures. Bottom line, it’s part of receiving and awarding federal and state grants.
Please click the button below to continue reading.
| |
|
Effective Advocacy for Survivors with Disabilities
Kelly Carpenter, Victims Services
Program Specialist
People with disabilities experience higher rates of assault and abuse than the general population yet are less likely to report the crime perpetrated against them[1]. The realities associated with various disabilities create vulnerabilities to sexual assault and abuse that are exploited by abusers[2]. Many people with disabilities need assistance with activities of daily living such as dressing, bathing, and toileting. Expected compliance with medical and therapeutic interventions can diminish the ability to understand, convey, or enforce personal boundaries. Hearing and/or speech differences can impact the ability to effectively communicate instances of abuse or assault. People with disabilities are often isolated due to lack of access or meaningful accommodations for inclusion in public spaces, and many services occur in segregated spaces away from peers. Further, access for people with disabilities to education and training around healthy relationships and sexuality is often minimal or missing altogether.
When these vulnerabilities are exploited and abuse occurs, people with disabilities face additional challenges to reporting these crimes and seeking healing and justice[3]. The realities that create vulnerabilities to assault and abuse may also be part of the barriers to reporting and accessing services. The good news is there are steps your agency can take to provide meaningful, accessible services for people with disabilities. As with any underserved or marginalized community, improving access and response takes intentional and coordinated efforts to reduce barriers.
This month, we are talking to Lisa Houck who is the Disability Services Coordinator for Project Horizon in Lexington, Virginia to discuss strategies for victim service organizations to help meet the needs of survivors with disabilities.
Please click the button below to continue reading the interview.
[1] https://bjs.ojp.gov/content/pub/pdf/capd0919st.pdf, retrieved 3/2/2023
[2] https://www.endabusepwd.org/heightened-risk/, retrieved 3/2/2023
[3] https://www.endabusepwd.org/about-the-movement/the-issue/, retrieved 3/14/2023
| |
|
Virginia Held its First Adult/Adolescent Sexual Assault Nurse/Forensic Examiner
Clinical Skills Lab
Gleibys Gonzalez, Sexual Assault Forensic Services Coordinator
In March 2023, Virginia held its first Adult/Adolescent Sexual Assault Nurse/Forensic Examiner Clinical Skills Lab at Valley Urgent Care in Harrisonburg, Virginia. The Clinical Skills Lab was sponsored by the DCJS Sexual Assault Forensic Examiner Coordinator Program in partnership with the International Association of Forensic Nurses (IAFN), the Office of the Attorney General, the Virginia Department of Health, and the Virginia Victims Fund.
The purpose of the Lab, as stated in the IAFN curriculum document, was: “to prepare the didactically trained SAFE/SANE for clinical aspects of the adult/adolescent sexual assault medical-forensic examination, regardless of the provider’s practice setting.”
To learn more about this training, please click the button below.
| | | |
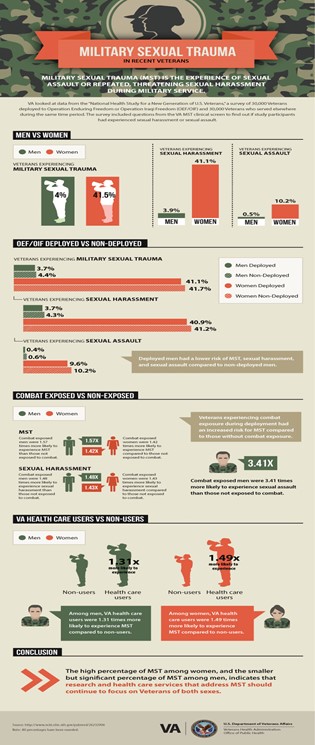
Combating Military Sexual Trauma (MST)
Tierra Williams, VSTOP & VSDVVF Grant Program Coordinator
According to the United States Department of Veterans Affairs (VA), military sexual trauma (MST) is sexual assault or sexual harassment experienced during military service (VA, 2023). Overall, it is characterized as any sexual activity that an individual may be involved with against their will. Examples of MST include sexual contact or activities without consent, being overpowered or physically forced to engage in sexual acts, unwanted sexual advances, or comments about one’s body or sexual activities that are perceived as threatening (VA, 2021). In a 2016 study conducted by the VA on men and women who served under the Operation Enduring Freedom or Operation Iraqi Freedom (OEF/OIF) eras, 4% of men and 41.5% of women indicated that they had experienced MST (VA, 2016). Moreover 3.9% of men and 41.1% of women responded that they had experienced sexual harassment, while 0.5% of men and 10.2% of women indicated they had experienced sexual assault (VA, 2016). The study also found that veterans who experienced combat exposure during deployment had an increased risk for MST compared to those without combat exposure (VA, 2016). In addition, screenings conducted by VA-based MST Support Teams across the nation revealed that 1 in 3 women and 1 in 50 men responded “yes” to experiencing MST (VA, 2021). Despite the numbers of experiences being higher for women than men, it is still vital that service providers continue to conduct research on this matter and address the needs of all individuals impacted by MST.
Veterans of different genders, races, and backgrounds have experienced MST. Impacts of trauma can manifest at any time even with adequate treatment and resources. For some individuals, MST can affect their mental and physical well-being in a multitude of ways. The type, severity, and duration of an individual’s difficulties may be influenced by various factors such as whether the individual has a prior history of trauma, the types of responses he/she received from others at the time of the MST, and whether the MST happened once or was repeated over time. In addition, cultural variables may also affect the impact of MST according to the VA (VA, 2021). Survivors of MST may have trouble sleeping, disturbing memories, self-doubt, feelings of isolation, sexual difficulties, difficulties in relationships, and issues with attention, concentration, and memory, among other obstacles that may impact their activities of daily living. Despite MST not being declared a mental health condition, chronic mental health diagnoses such as posttraumatic stress disorder (PTSD), substance abuse, depression, and other mood disorders are often associated with MST (VA, 2021). Although the reactions men and women have to MST are similar in some ways, they may also struggle with different issues making it necessary to provide a tailored treatment plan geared towards each survivor’s unique needs and recovery plan.
MST is considered an experience and not a diagnosis or mental health condition (VA, 2021), however the physical and mental impacts of MST warrant the need for services that provide support and adequate intervention. With the prevalence of MST, the VA endorses they are “…strongly committed to ensuring MST survivors have access to the help they need in order to recover” (VA, 2021). All treatment for physical and mental conditions related to MST are free to veterans and evidence-based treatment is widely available as well. MST specific services are available at every VA medical center and MST counseling is also available through community-based Vet centers. Mental health services include psychological assessments, medication evaluation and individual or group therapy. To accommodate Veterans who do not feel comfortable in mixed-gender treatment settings, some facilities even offer separate programs for men and women. To respond to the impact of MST, the VA healthcare system also has designated MST Coordinators who serve as the premier point of contact exclusively for MST-related issues. The coordinator is responsible for aiding individuals in locating and accessing VA services and programs designed to address MST. Nationwide, there are also residential or inpatient services available for survivors who may need more intense treatment. The VA has also launched the Beyond MST App, which is a free, trauma-sensitive app that has over 30 specialized tools that help users to cope with challenges, manage their symptoms, and track recovery (VA, 2023). Whether in a residential or community-based setting the VA continues to offer a multitude of supports and treatment options to promote many paths to healing.
It’s important to know that MST can occur on or off base, during war or peacetime, and while a Service Member is on or off duty. For more information, Veterans can speak with their existing VA health care provider, contact the MST Coordinator at their nearest VA medical center, or contact their local Vet Center. A list of VA and Vet Center facilities can be found at www.va.gov and www.vetcenter.va.gov.
| | | | | |