President's Message
Valued ACHA Certificant Holders,
I hope you had a fantastic time reconnecting with colleagues and friends at the 2024 ASHE PDC Summit in sunny San Diego. The sessions were informative, and the networking opportunities were plentiful.
I'm excited to share some important updates:
- New "Think Tank" Initiatives: We're exploring ways to leverage the expertise of our client-employed certificant holders. Soon we will form a new "Think Tank" that will focus on communicating the value of having ACHA-certified architects on design teams to healthcare organizations. Reach out to me if you are interested in being part of this group. Our AI Think Tank is already hard at work.
- ACHA Student Competition Expansion: Preparations are in progress to expand the reach and impact of the 2024-2025 ACHA Student Competition which was so successful in its inaugural year .
- ACHA Emeritus Status Update: We have revised our requirements for ACHA Emeritus status. These are posted on our website.
- ACHA / AIA AAH Collaboration: Working with the AIA Academy of Architecture for Health (AIA AAH), we established a policy for recognizing newly deceased distinguished members of both organizations at the annual Summer Leadership Summit. This information has been posted to our website as well.
-
ACHA Exam Preparation: For those candidates who are preparing for the ACHA Exam in June, let us know if you are interested in an Exam Study Group. If so, e-mail Emily.Brochstein@kellencompany.com and we will connect everyone.
| |
Join us in Denver
I look forward to seeing you in Denver, Colorado, for the ACHA/AIA AAH Summer Leadership Summit on July 26-27, 2024. Dive deep into the "Health and Healthcare in an AI Future" theme exploring the exciting ways Artificial Intelligence is transforming our field. Denver's stunning mountain scenery provides the perfect backdrop where you can learn, network, and be inspired! The ACHA luncheon for the first time will include the induction of Class of 2024 Fellows. Early bird registration opens in May.
I'm eager to connect with you in Denver. Feel free to reach out to me at ann.adams@davispartnership.com anytiing me for any reason.
Let's make this a year to remember!
Ann H. Adams, AIA, FACHA
ACHA President
| |
PDC San Diego Recap
The American Society for Health Care Engineering (ASHE)’s 2024 PDC Summit in San Diego was eventful for ACHA! Certificants connected with their peers at the ACHA booth and also led and attended countless panel discussions on topics ranging from AI's impacts to hospital decarbonization.
The PDC Summit allows healthcare professionals across architecture, engineering, and other stakeholders to meaningfully collaborate and address the evolving needs of patients, and healthcare providers. We are proud to be a supporting organization and thankful to all who offered their insights and made this such a memorable event!
Session and event highlights, featuring College certificants:
-
Opening Session / Keynote: Shola Richards, Founder & CEO, Go Together Global & Best-Selling Author provided an inspirational message to kick-off the conference by introducing the concept of UBUNTU: I am because we are. Relying on past personal experiences he challenged the audience to transform their work culture, amplify team civility, and inspire themselves to bring their best to their work. He suggested applying three tests of evaluation to help guide correct decisions and direction: 'is it kind' – be the person who people feel better when you walk into the room instead of out of it; ‘is it time’ – apply the metrics of the appropriateness of attitude and voice relative to the situation; ‘is it necessary’ – reimagining resilience by realizing problems won’t get better, address and commit. Practicing these tenants individually will only help the greater good, and by doing the right thing ‘just today’ (tomorrow is not promised) we can have a positive effect on everyone's experiences.
-
Medical Equipment and Technology Integration Forum (with focus on Lab Planning, ft Lisa Charrin, AIA, ACHA): Focus on the Implementation of Lean planning theories to maximize efficiencies for time-dependent tests and flows. Inventory process for understanding current state, flexibility and opportunities for reuse is critical, including considerations for phasing or moving. Practice the use of flexible benches, 30-36” depths, often with equipment coming with additional accessories, printers, computers, etc. and a mix of wet and dry systems. Automation integration and digitation planning is important - digital pathology, accessioning, staining, etc. Consistent power and UPS are mandatory for success and resilience on power interruptions. Structure is driven directly by equipment specifications and vibration requirements, including advance planning for slab depressions for walk in coolers, etc. There continue to be high first costs of equipment for specimen movement versus courier reliance, with increasing opportunities for robotics and the importance of tracking these valuable specimens. Plan for science and equipment to change, including sizing extra vertical infrastructure - give room in chases.
-
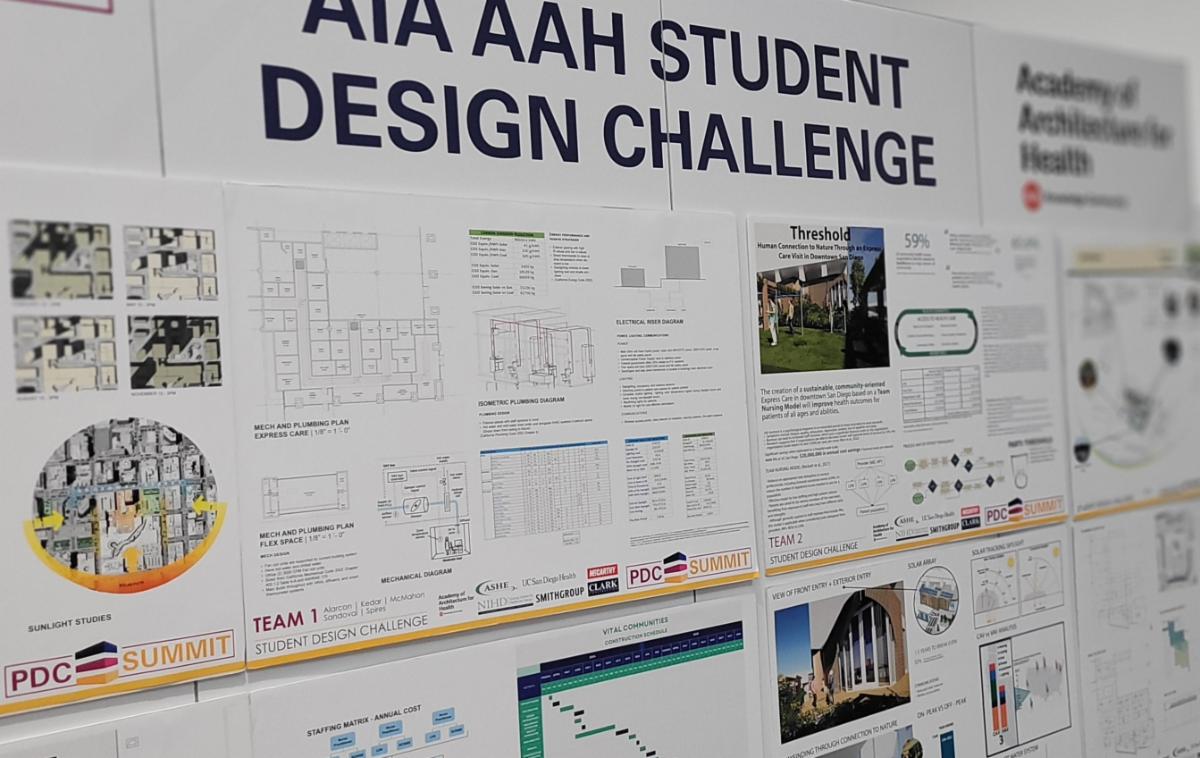
AIA/AAH PDC Student Challenge (sponsored by ACHA): 10-person Jury, the ACHA was represented by Ted Moore, ACHA, Haskell; David Allison, FACHA also participated as the Clemson Faculty Advisor. This was a 48-hour charrette, consisting of multi-disciplinary teams made from representatives from University of Florida, Montana State, Milwaukee school of Engineering, University of Washington, Clemson (nursing, engineering, design, and construction fields represented in each cohort team). The program was a San Diego- based under-utilized urban site located 10 minutes from the convention center. The goal was a carbon neutral 10-exam room urgent care facility that is operationally efficient, resilient. 4,300 SF and adjacent exterior space. Juror comments on the winner and runner-up:
o Second place “Threshold” - Considered staff turnover as financial incentive for the design. Transitional space between nature and building, extending space out into community and nature. Emphasis on the patient experience with views to nature, light penetrating building, equitable care and resources for healing beyond physical care. Solar and natural lighting are used to extend sustainability, and solar panels used to heat the water. A design-build approach was planned to meet occupancy schedule.
o First place winner “Gateway to Health” – The solution was an extension of a gateway into the community. Took advantage of site orientation for lighting and location in the community for transit and access along a natural pedestrian path. The team used lean planning and spaghetti diagrams to test flows with different patient personas facing different needs and diagnosis. The solution Includes a negative pressure room and UV sterilization to maximize infection prevention. Acoustical strategies were implemented to maximize patient privacy in exam rooms.
-
Navigating the Labyrinth of Health Care Codes (ft Tina Duncan, AIA, ACHA) - Healthcare reimbursement is dependent on being safe and compliant with codes, thus the importance. Most important and influential continue to be NFPA 101, NFPA 99, IBC, model codes and standards, FGI, ADA, etc. NFPA 101 Life Safety Codes are still 2012 edition as recognized by CMS – this forces a least common denominator, minimum, and occupancy-based approach. Residential Board and Care (may include unlocked behavioral health facilities) and Business Occupancies both rely on prompt evacuation as opposed to defend in place strategies. NFPA 99- Healthcare Facilities Code, 2012 edition for CMS-deemed facilities, but Chapter 5, 6, 9,10, 11, 14, 15 were the only adopted chapters (note IT, Plumbing, Emergency Management and Security Management were chapters not adopted). This is a risk-based document, risk assessment required to determine category application and extent of redundancy for different systems. IBC is currently working to better align with Life Safety Codes. The 2022 FGI Guidelines is the current edition (or state adopted rules) and is adopted in some form in 43 states, and focuses on programming, space planning and allocated, healthcare design criteria. Many states on older versions (like Kansas, using 96-97 as minimum standard) may allow newer editions but may also require an analysis of “most restrictive” code language. ADA and A117.1 are typically used for accessibility. Everything is required to be accessible unless it is an exception (including staff toilets). ANSI A117.1 is enforced by building inspectors. ADA is federal, enforceable through the DOJ and torts.
-
How Design Standards Drive Innovation – perspectives given from Design (Kaiser Permanente), Engineering (Mazzetti), Owner (Stanford Health), and Construction (Bolt). A recognition of the difference of standards (have to use) vs guidelines (suggested use) is important to understand the specifics of integration. Kaiser started the standardization process through their ‘Small Hospital, Big Idea’ competition in 2011, with an emphasis on providing the right care at the right time in the right place. There are financial incentives to standardize, evidenced by a change from 24 bed units to 36 beds that resulted in $36k / year in operational savings systemwide. It is important to update clinical standards every 3 years. From a deign perspective they placed a reliance on fully informed templates to fit into a kit of parts (changing Architecture to ‘modutecture’). From the engineering perspective, standards = automation. Simplify complexity with a standardized kit of parts. A robot is only as good as it’s handler. Focus on simplification and streamlining for innovation. From the Owner’s perspective, a case study on an on-campus MOB was used to illustrate how timing and creative thinking could help with requirements. A two-year hold allowed the parking standards to be re-evaluated due to the change in how users arrived at a facility (the Uber effect), resulting in an agreed-to revision in parking ratio requirements. There was some need to align existing standards to the structural grid – some room templates were not as flexible, resulting in an irregular grid. Mockups and modular walls are essential – non-standard sizes are 2-3x more expensive. In a response to telemedicine demands, some exam rooms were needed to be converted allowing a two to one switch to more of an office setting (this was done over a weekend). Finaly, from the Construction view in an integrated process, evidence-based design is equated to design and process standards. Assistance with fabrication and integrated design borne through codes, resulting in product standards – ‘building configurator’. Create a catalogue ‘look book’ of select elements of the design; this could cut costs by ½ vs using specialized solutions. Creating digital twins through technology for modeling helped increase accuracy of as-builts and inventory assets.
-
PDC Hacks for the Patient Experience – An Owner and Architect shared their thoughts on ways to improve the wholistic patient journey beyond just the immediate care areas. Using responses from HCAHPS surveys and other requested intelligence, there were nine identified ‘hacks’ to allow a facility to more effectively present a positive experience (understanding that personnel have a profound impact – a happy employee = a happy patient). 1) Carefully plan and position elevators for organization and separation, assisting in patient, staff, materiel flow and clarity. 2) Entry points – position thing along the way to know where you are going (using city planning from Rome as an example of how elements and specific path widths, etc can assist). 3) Mind your main streets – doesn’t have to be a straight line but create a direct route. 4) Wayfinding – proper, logical, clear: we don’t need more signs. 5) Think about the ease of cleaning; the devil is in the details. Don’t create more to clean. 6) Mind what is at the front door – am I in the right place? Logic and clarity of space with less clutter. 7) Neat and tidy barriers in construction. Commitment to cleanliness and an opportunity to promote the new area. 8) Plan out the noise in construction – set timeframes for work and quiet hours. If you are not expecting, it hurts. 9) Communicate with care staff – someone will hear it on the 100th time. Provide updates, use staffing huddles, allow for questions.
| | |
|
Next Town Hall – Health Equity
Join us for the next ACHA Town Hall, May 15 from 4-5pm EDT. When contemplating the forces currently influencing healthcare design, the discussion includes health-related diversity, equity and inclusion (DEI). DEI has impacted many aspects of our community from the use of technology to shifts in work force demographics and how we collaborate. As healthcare architects and designers, we strive to make a positive contribution to healing environments and an understanding of health equity is key to effective design.
| |
BD+C, ACHA partner for “Outpatient Facilities Survey 2024”
Building Design+Construction and ACHA are partnering on an important research initiative – the “Outpatient Facilities Survey 2024.” As you know, outpatient facilities and medical-dental office buildings now account for $18.2 billion in annual construction – 42% of all healthcare construction spending.
| | |
Save the Date - Summer Leadership Summit
July 26–28 | Denver | Grand Hyatt Denver
Emerging technologies such as artificial intelligence (AI), augmented reality, and virtual reality (VR) impact health care, the architecture profession, and communities every day in exciting and potentially concerning ways. As our world becomes more virtual, and artificial, how do we stay grounded in reality? How will our institutions harness these new technologies to impact health outcomes?
| |
|
Candidate Exam Incentive
In an effort to entice potential applicants into the College, ACHA is excited to announce that, starting in 2023, any ACHA applicant who passes the certification exam can receive 20 AIA-approved HSW CEUs for the testing year. This will satisfy a substantial portion of CEUs required for architectural licensure in most states. Candidates will then be well on their way to ACHA certification with the added benefit of reduced cost for achieving educational requirements!
| |
|
Call for Certificant News
We want to know what the members are doing to promote the College! If you know of or are involved in upcoming events, seminars, symposiums, or promotions, please email the editor, Neal Corbett.
| | |
[913-222-8653] [acha-info@kellencompany.com] [healtharchitects.org] | | | | | |